
Insulin resistance usually cannot be cured with one food, supplement, or short reset. If you are searching for how to cure insulin resistance, the practical answer is to improve insulin sensitivity through sustainable eating patterns, regular activity, sleep, weight-related care when relevant, and medication when a clinician recommends it. This matters because insulin resistance can precede prediabetes, type 2 diabetes, fatty liver disease, and cardiovascular risk factors, even before symptoms feel obvious.
Key Takeaways
- No instant cure: Insulin sensitivity can improve, but quick fixes are unreliable.
- Food quality matters: Fiber-rich carbohydrates, protein, and unsaturated fats often support steadier glucose.
- Movement helps: Aerobic activity and resistance training can make muscles more responsive to insulin.
- Symptoms may be subtle: Some people notice skin, energy, menstrual, or weight-related changes.
- Medical review helps: Lab trends and risk factors guide treatment choices.
How to Cure Insulin Resistance Without a Quick Fix
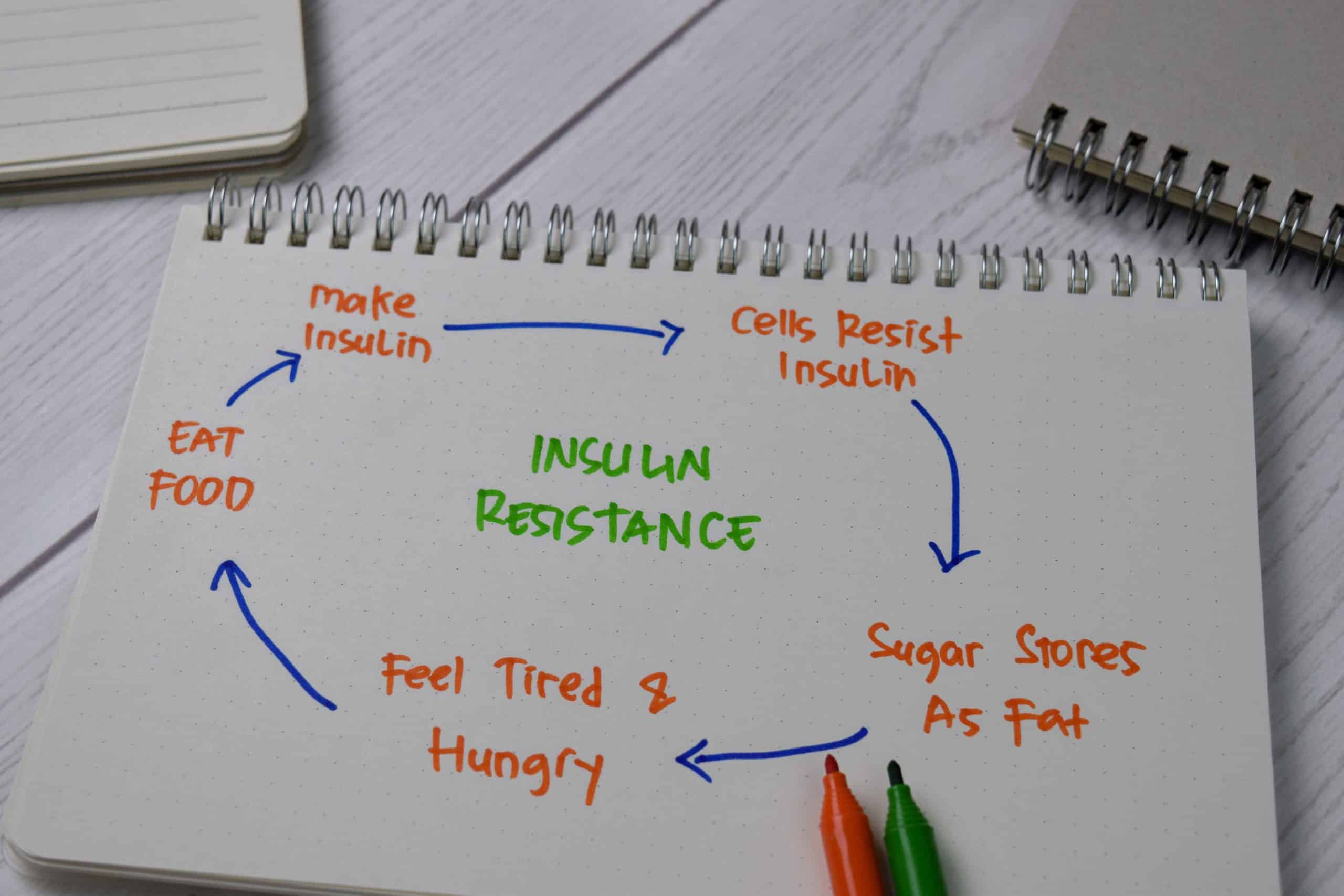
Insulin resistance means your cells respond less effectively to insulin, the hormone that helps move glucose from the bloodstream into cells. The pancreas may compensate by making more insulin. Over time, this higher insulin demand can strain glucose control and raise the risk of prediabetes or type 2 diabetes.
A realistic answer to how to cure insulin resistance starts with the word improve. Some people can bring insulin sensitivity and blood sugar markers back into healthier ranges. Others can reduce risk and slow progression, even if a tendency toward insulin resistance remains. The difference depends on genetics, body composition, sleep, medications, hormones, age, pregnancy history, and other conditions.
It also helps to separate insulin resistance from diabetes. Insulin resistance can exist before blood sugar reaches the diabetes range. That early window is important because daily habits may have a stronger effect before long-term beta-cell strain develops. For a broader primer, see Insulin Resistance Signs.
Why it matters: Treating insulin resistance as a pattern, not a single lab result, supports better follow-up.
What Insulin Resistance Can Feel Like
Insulin resistance often has no clear symptoms at first. Many people learn about it after routine blood work shows rising fasting glucose, A1C, triglycerides, or other metabolic changes. Others notice signs that can overlap with many conditions, so symptoms alone cannot confirm the diagnosis.
Possible clues include increased waist size, tiredness after meals, frequent hunger, difficulty losing weight, high blood pressure, abnormal cholesterol patterns, skin tags, or dark velvety skin patches called acanthosis nigricans. People should seek medical review for excessive thirst, frequent urination, unexplained weight loss, blurry vision, recurrent infections, or symptoms of very high blood sugar.
Insulin resistance symptoms in females can include the same general signs. They may also appear alongside polycystic ovary syndrome, or PCOS, which can involve irregular periods, acne, increased facial hair, or fertility concerns. These symptoms deserve individualized assessment because thyroid disease, pregnancy, menopause, medications, and eating patterns can also affect weight, energy, and cycles.
Clinicians may use fasting glucose, A1C, lipid tests, blood pressure, waist measures, medication history, family history, and sometimes fasting insulin. Fasting insulin and HOMA-IR can provide context, but they do not diagnose every person on their own. If you are reviewing fasting glucose and fasting insulin with a clinician, this calculator can help organize the general estimate.
HOMA-IR Calculator
Estimate insulin resistance from fasting glucose and fasting insulin values collected from the same blood draw.
These calculations are for education only and do not replace clinical advice, diagnosis, or treatment. Always confirm medical decisions with a qualified healthcare professional.
The calculator estimates HOMA-IR from fasting glucose and fasting insulin. It should support a conversation, not replace medical interpretation.
If you are trying to understand glucose results, the Blood Sugar Range Chart explains common numbers in plain language.
Food Choices That Support Better Insulin Sensitivity
An insulin resistance diet is not one rigid plan. The most useful pattern usually reduces large glucose swings while still providing enough nutrition, satisfaction, and flexibility. Many people do better when meals include fiber-rich carbohydrates, lean or minimally processed protein, unsaturated fats, and non-starchy vegetables.
Carbohydrate quality matters. Whole grains, beans, lentils, fruit, yogurt, and starchy vegetables can fit many eating patterns when portions and pairings are considered. Sugary drinks, frequent desserts, refined snack foods, and large portions of low-fiber starches can make glucose control harder for some people. Individual responses vary, especially with sleep, stress, activity, and medications.
Simple meal-building principles often help more than strict food rules:
- Start with plants: Add vegetables, beans, lentils, or whole grains.
- Pair carbohydrates: Include protein or healthy fat with starches.
- Watch liquids: Sweet drinks can raise glucose quickly.
- Read labels: Compare fiber, added sugar, and serving size.
- Plan repeat meals: Familiar meals make tracking easier.
A 7-day insulin resistance diet or 30-day meal plan can be useful for practice, but it should not be treated as a cure. The goal is to learn which meals keep you full, fit your culture and budget, and support better lab trends over time. If you use insulin or medicines that can cause low blood sugar, changing carbohydrate intake should be discussed with your clinician.
A registered dietitian can be especially helpful during pregnancy, kidney disease, gastroparesis, eating disorder recovery, recurrent hypoglycemia, or major medication changes. For related nutrition and weight-management context, see Diabetes Weight Loss.
Movement, Sleep, and Weight Changes That Shift Risk
Physical activity improves insulin sensitivity because working muscles use glucose more readily. This effect can happen even before major weight change. Aerobic exercise, resistance training, and less sitting all support metabolic health in different ways.
You do not need a perfect routine to start. Walking after meals, climbing stairs, cycling, swimming, strength training, or home-based resistance exercises may all help. The safer starting point depends on your fitness level, joint health, heart risk, glucose medications, and any diabetes complications. People with chest pain, severe shortness of breath, fainting, or new neurological symptoms should seek urgent medical care.
Sleep and stress deserve attention because they affect hormones, appetite, glucose regulation, and consistency. Short sleep, untreated sleep apnea, shift work, chronic stress, and depression can make insulin resistance harder to manage. These factors are not character flaws. They are medical and environmental pressures that often need practical support.
Weight change can improve insulin sensitivity for some people, especially when excess visceral fat is present. Still, insulin resistance is not only a weight issue. People in smaller bodies can have insulin resistance, and people in larger bodies can improve metabolic markers without reaching a specific weight. A useful plan focuses on labs, blood pressure, waist measures, strength, energy, and sustainable behaviors.
For more detail on daily changes that may help, review Improving Insulin Sensitivity.
When Treatment Includes Medication
Insulin resistance treatment depends on the full health picture. Lifestyle changes are central, but medication may be appropriate when blood sugar, A1C, PCOS, weight-related risk, or type 2 diabetes risk requires more support. Medication decisions should come from a licensed clinician who can review kidney function, pregnancy status, other prescriptions, side effects, and goals.
Metformin for insulin resistance is a common search because metformin can reduce liver glucose production and improve glucose control in certain groups. It is widely used for type 2 diabetes and may be considered in some people with prediabetes risk factors or PCOS, depending on clinical circumstances. It is not a do-it-yourself treatment, and it is not the only possible option.
Other medicines may be used when someone has type 2 diabetes, obesity, cardiovascular risk, or other indications. Some drug classes affect appetite, weight, glucose absorption, insulin secretion, or insulin sensitivity. The right choice depends on diagnosis, contraindications, tolerability, cost, access, pregnancy plans, and monitoring needs. For a deeper medication-focused overview, see Insulin Resistance Treatment.
Some people with insulin resistance eventually need insulin or other injectable medicines. That does not mean they failed. It usually means the pancreas, liver, muscles, fat tissue, and hormones need more support than lifestyle changes alone can provide. Never stop, start, or adjust diabetes medication without medical guidance.
For access questions after a clinician prescribes treatment, CanadianInsulin.com acts as a prescription referral platform.
Supplements, Natural Remedies, and Common Pitfalls
The safest answer to how to cure insulin resistance rarely starts with a supplement. Some supplements, spices, or herbal products are marketed for glucose control, but evidence quality varies, product strength can be inconsistent, and interactions can occur. This is especially important if you take diabetes medication, blood thinners, blood pressure medicine, fertility treatment, or are pregnant.
Natural remedies for insulin resistance should be judged by the same standard as any treatment: benefit, risk, dose uncertainty, interactions, and monitoring. Magnesium, vitamin D, cinnamon, berberine, and other products may be discussed online, but none should replace nutrition changes, activity, sleep care, or prescribed treatment. A clinician can also check whether a deficiency is present before supplementation.
Common pitfalls include:
- Chasing speed: Fast reversal claims often oversimplify biology.
- Cutting too hard: Extreme restriction can backfire or trigger lows.
- Ignoring sleep: Poor sleep can worsen cravings and glucose patterns.
- Skipping follow-up: Lab trends show more than symptoms alone.
- Overusing supplements: More products can mean more interaction risk.
Quick tip: Bring supplement bottles or photos to appointments for safer review.
How to Tell Whether Insulin Resistance Is Improving
Signs insulin resistance is reversing are usually seen through trends, not one perfect number. Fasting glucose, A1C, triglycerides, HDL cholesterol, blood pressure, waist measures, liver enzymes, and medication needs may all provide clues. Some people also notice steadier energy, fewer cravings, improved cycles in PCOS, or less pronounced acanthosis nigricans, though these changes are not guaranteed.
Home glucose checks can help some people understand patterns, especially after meals. They are most useful when your clinician explains when to test, what range matters for your situation, and how to respond safely. The article Blood Sugar Monitoring covers common monitoring considerations.
High insulin levels can improve before blood sugar changes become obvious, but insulin tests are not always part of routine care. If fasting insulin is measured, it should be interpreted with glucose, A1C, lipids, waist measures, and risk history. The related overview on High Insulin Levels explains why context matters.
Insulin resistance also overlaps with metabolic syndrome, a cluster that may include high blood pressure, abnormal cholesterol, elevated glucose, and increased waist circumference. Understanding that pattern can help you ask better follow-up questions. See Metabolic Syndrome for more background.
If your main goal is how to cure insulin resistance, treat it as a long-term risk pattern that can often improve. Ask your clinician which markers matter most, how often to repeat labs, whether medication is appropriate, and when symptoms should prompt faster review. You can also browse the Type 2 Diabetes Articles hub for related education.
Authoritative Sources
- The CDC explains insulin resistance and type 2 diabetes.
- The American Diabetes Association reviews insulin resistance basics.
- The NICHD summarizes PCOS symptoms and related risks.
Insulin resistance can improve, but progress is usually gradual and individual. The most useful plan combines realistic food changes, movement, sleep support, medical follow-up, and treatment when indicated.
This content is for informational purposes only and is not a substitute for professional medical advice.


{kind=link}
{kind=link}