
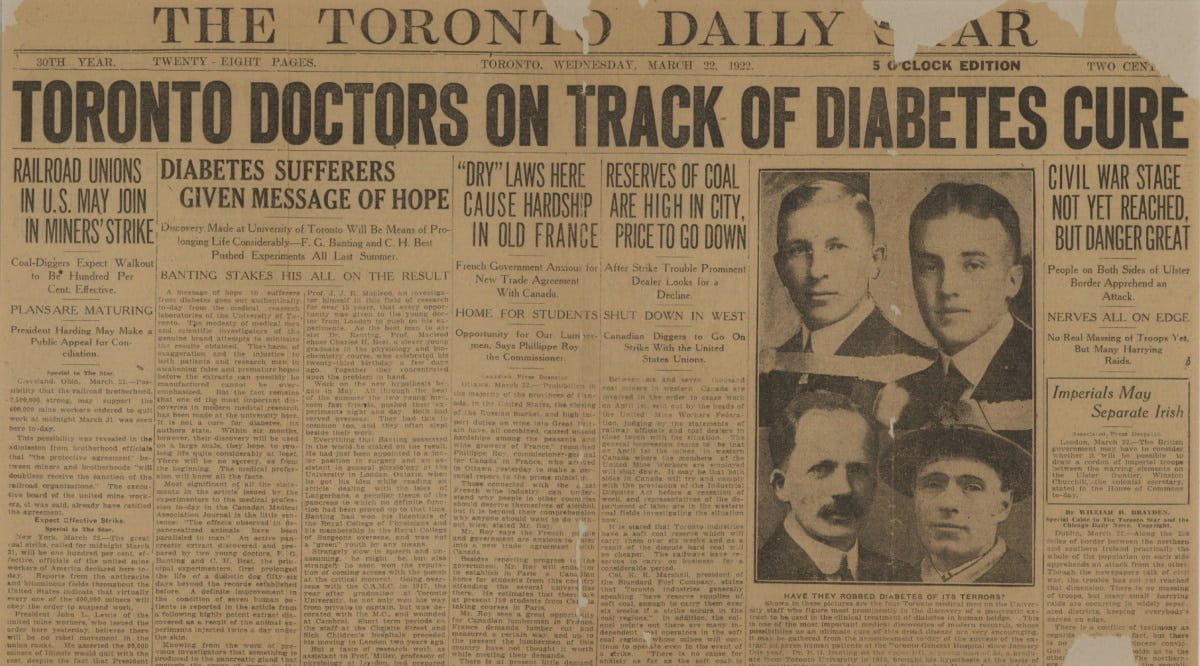
The discovery of insulin began with a clear medical problem: people with severe diabetes were dying because their bodies could not use glucose properly. In 1921, a Toronto research team isolated a pancreatic extract that lowered blood sugar in animals, then refined it for human use in 1922. That work turned type 1 diabetes from a usually fatal condition into a treatable chronic disease.
This history matters because insulin is still central to diabetes care. It also explains why scientific credit, manufacturing, patents, and access remain part of the public discussion.
Key Takeaways
- Major turning point: Insulin changed severe diabetes care.
- Shared work: Banting, Best, Macleod, and Collip all contributed.
- First patient: Leonard Thompson received refined extract in 1922.
- Production changed: Modern insulin usually uses recombinant DNA methods.
- Access debate: Early patent choices still shape ethical discussions.
How the Discovery of Insulin Happened
The discovery of insulin was not a single accident. It followed decades of evidence that the pancreas played a key role in diabetes. In 1889, Oskar Minkowski and Joseph von Mering found that removing the pancreas from dogs caused diabetes-like symptoms. In 1910, Edward Sharpey-Schafer proposed that the pancreas released a missing substance, later associated with the name insulin.
Frederick Banting, a Canadian surgeon, built on those ideas. He believed that pancreatic tissue might be treated in a way that preserved the internal secretion needed to lower blood sugar. In 1921, he began work at the University of Toronto with medical student Charles Best. John Macleod provided laboratory space, scientific oversight, and access to animals and equipment.
Banting and Best tested pancreatic extracts in dogs whose pancreases had been removed. The crude extracts lowered blood glucose, but they were not yet safe or reliable enough for people. James Collip, a biochemist, then improved the purification process. His work made the extract more suitable for clinical testing.
Why it matters: The breakthrough required both a bold hypothesis and careful purification.
For readers who want a shorter companion piece, our related page on Insulin Discovery gives a compact overview of the same historical turning point.
Diabetes Before Insulin: What Treatment Looked Like
Before insulin, severe diabetes was usually managed with strict food restriction. Physicians used fasting, very low-calorie diets, and limited carbohydrates to reduce sugar in the urine. These approaches sometimes delayed decline, but they did not correct the underlying hormone deficiency.
Children and young adults with what is now called type 1 diabetes faced especially poor outcomes. Many lost weight, became weak, and developed life-threatening complications. Doctors could measure sugar in urine, but they had no treatment that replaced the missing pancreatic hormone. Care often focused on keeping patients alive for as long as possible.
Elliott P. Joslin and other early diabetes physicians carefully documented diet-based management. Their records showed that discipline and monitoring could help some patients survive longer. Still, these methods carried serious tradeoffs, including malnutrition and exhaustion. The arrival of insulin changed the goal of treatment from slowing decline to restoring a more workable metabolism.
Modern care differs sharply from that era. People now learn about glucose monitoring, carbohydrate intake, insulin timing, and long-term complication prevention. For broader educational context, the Type 1 Diabetes collection groups related resources for readers exploring diagnosis and care concepts.
First Human Use: Leonard Thompson and the 1922 Trial
Leonard Thompson, a 14-year-old with severe diabetes, became the first person treated with the Toronto extract. He received an initial injection in January 1922 at Toronto General Hospital. That first attempt produced limited benefit and caused reactions, likely because the extract still contained impurities.
Collip then refined the preparation further. A later course produced a much stronger clinical response, including lower glucose readings and visible improvement. This moment became one of the most important milestones in the history of insulin because it showed that a pancreatic extract could work in a human patient.
The team soon treated more patients. Reports spread quickly among physicians, families, and hospitals. Demand increased because the therapy addressed a condition that had few meaningful options. Scaling production became urgent, and pharmaceutical partners helped standardize extraction, potency testing, and supply.
Early insulin came from animal pancreases, mainly bovine and porcine sources. That was practical because slaughterhouses could supply pancreatic tissue. Animal insulin saved lives for decades, although purity, immune reactions, and consistency remained important concerns. Our discussion of Animal Insulin Types explains how those earlier preparations differ from many current products.
Who Deserves Credit for Insulin?
Credit for the discovery of insulin is shared because the work depended on several roles. Banting proposed the experimental approach and drove the early project. Best worked closely with him in the laboratory. Macleod supplied the research setting, helped interpret findings, and guided the scientific process. Collip purified the extract enough for successful human treatment.
The Nobel Prize in Physiology or Medicine was awarded in 1923 to Banting and Macleod. Banting shared his prize money with Best. Macleod shared his portion with Collip. That choice reflected the reality that the achievement was collaborative, even though tensions remained over priority and recognition.
The controversy continues because different accounts emphasize different parts of the work. Some focus on Banting and Best’s animal experiments. Others stress Macleod’s laboratory leadership or Collip’s purification step. A fair reading recognizes that the therapy would not have reached patients safely without the combined effort.
The question “who invented insulin” also needs careful wording. Insulin is a naturally occurring hormone. The Toronto team did not invent the hormone itself. They developed a usable therapeutic extract and helped move it from animal experiments to clinical care.
What Insulin Does in the Body
Insulin helps move glucose from the bloodstream into cells, where it can be used or stored. It also helps regulate how the liver releases glucose between meals. When insulin is absent or insufficient, blood glucose can rise, and the body may start breaking down fat and muscle for energy.
In type 1 diabetes, the immune system destroys insulin-producing beta cells in the pancreas. In type 2 diabetes, the body may resist insulin’s effects, and insulin production may decline over time. These conditions differ, but both can involve problems with insulin availability, action, or both.
The structure of insulin also became scientifically important. Insulin is a protein hormone made of two linked chains of amino acids. Later work showed that understanding its sequence and shape could improve manufacturing, purity, and modification. This helped open the way for human insulin, analog insulin, and biosimilar insulin development.
For a care-context comparison, our page on Human Insulin vs Analog Insulin explains broad differences between conventional human insulin and modified analog formulations.
How Insulin Is Produced Artificially Today
Modern insulin production usually relies on recombinant DNA technology. Manufacturers insert the genetic instructions for human insulin into microorganisms such as bacteria or yeast. Those cells produce insulin or insulin precursors, which are then purified, processed, and formulated.
This approach replaced heavy reliance on animal pancreases in many settings. It allows more consistent large-scale production and avoids some animal-source limitations. It also supports the creation of insulin analogs, where small structural changes adjust onset, peak, or duration.
People often ask, “is insulin made from pigs?” Historically, porcine insulin was common. Some animal-derived products still exist in limited settings, but many current insulins are recombinant human insulin or analogs. Product choice depends on clinical needs, regulatory approval, access, and prescriber judgment.
Our explainer on Synthetic Insulin Made gives more detail on artificial production methods. Readers comparing newer follow-on products can also review Biosimilar Insulin for general background on similarity, regulation, and use.
From Extracts to Modern Delivery
Early insulin treatment required reusable glass syringes and needles that needed careful cleaning. Dosing decisions were less flexible, and glucose monitoring was far more limited than it is today. Over time, insulin formulations, syringes, pens, pumps, and glucose sensors changed daily diabetes management.
Short-acting, intermediate-acting, and long-acting preparations helped clinicians match insulin action to meals and baseline needs. Later analogs offered additional options, although no formulation is right for every person. Decisions depend on diagnosis, glucose patterns, hypoglycemia risk, daily routine, cost, and access.
Some readers may want examples of current insulin categories. Regular human insulin products, such as Humulin R Vial, are one type used in certain treatment plans. Rapid-acting analog examples include Humalog Vial, while long-acting basal options include products such as Lantus Vial. These links are for product context, not treatment selection.
CanadianInsulin.com is a prescription referral platform, and prescription details may be confirmed with a prescriber where required. Dispensing and fulfilment are handled by licensed third-party pharmacies where permitted. That access context is separate from the historical evidence reviewed here.
Insulin Patent History and Access Debates
The insulin patent story is central to the discovery’s legacy. Banting, Best, and Collip assigned patent rights to the University of Toronto for a token amount. Their aim was to prevent personal profiteering and help make production broadly available through controlled licensing.
This decision is often summarized by the phrase that insulin belongs to the world. The phrase captures the ethical spirit of the early team, although manufacturing still required infrastructure, quality control, and regulation. As insulin products evolved, access debates became more complex.
Modern affordability discussions involve many factors, including production, distribution, insurance design, market structure, and national policy. Historical patent choices do not fully explain today’s costs. Still, they remain important because they show that public health and scientific credit were linked from the beginning.
For readers navigating broader diabetes resources, the Diabetes collection provides educational material across treatment, monitoring, and condition basics. The Diabetes medical-condition page can also help readers browse related product categories and condition-linked listings.
History of Insulin Timeline
A timeline helps separate early clues, the Toronto breakthrough, and later manufacturing milestones. The discovery of insulin sits in the middle of a longer story that includes physiology, protein chemistry, biotechnology, and regulation.
- 1889: Minkowski and von Mering link the pancreas to diabetes in dogs.
- 1910: Sharpey-Schafer proposes a missing pancreatic substance later tied to insulin.
- 1921: Banting and Best test pancreatic extracts in Toronto laboratory animals.
- 1922: Leonard Thompson receives refined extract at Toronto General Hospital.
- 1923: Banting and Macleod receive the Nobel Prize and share credit.
- 1950s: Protein sequencing work clarifies insulin’s amino acid structure.
- 1970s-1980s: Recombinant DNA methods support human insulin production.
- Later decades: Analog insulins, pens, pumps, and glucose sensors expand care options.
This sequence also answers whether insulin was discovered by accident. Chance did not drive the result alone. The breakthrough came from prior evidence, a testable idea, animal experiments, purification, and rapid clinical translation.
Authoritative Sources
Historical medical topics benefit from primary or expert-backed references. The Nobel Prize 1923 summary documents the award and its formal recognition of Banting and Macleod.
The FDA’s historical exhibit, 100 Years of Insulin, provides regulator-backed context on the therapy’s development and production history.
For a peer-reviewed historical review, see this open-access article on insulin as a medical milestone, which summarizes key scientific and clinical developments.
Recap
The discovery of insulin changed diabetes care because it replaced starvation-based management with hormone replacement. The Toronto work was fast, but it was not simple. It drew on earlier physiology, careful animal experiments, chemical purification, hospital testing, and urgent production scale-up.
The legacy is still active. Modern insulin is usually made through biotechnology, delivered through improved devices, and discussed within broader questions about access and affordability. Historical summaries simplify complex events, so readers should compare credible sources when evaluating credit, timelines, and controversy.
This content is for informational purposes only and is not a substitute for professional medical advice.

{kind=link}
{kind=link}