
An insulin pump is a wearable device that delivers rapid-acting insulin through a small tube or patch under your skin. For readers looking for an Insulin Pump: How It Works, Types, and Patient Guide, the short answer is that pump therapy replaces repeated daily injections with programmed background insulin and on-demand meal doses. It can add flexibility for some people, but it also requires training, site care, and a backup plan if insulin delivery stops.
Key Takeaways
- Most pumps deliver only rapid-acting insulin.
- They provide basal insulin all day and bolus doses for meals.
- Common formats include tubed, tubeless, and automated systems.
- Pump therapy may suit both type 1 and some type 2 diabetes cases.
- Interrupted delivery can raise ketone and ketoacidosis risk.
How an Insulin Pump Works
An insulin pump gives insulin by continuous subcutaneous insulin infusion, which means small amounts of insulin move under the skin throughout the day. Instead of taking separate long-acting insulin, the device is programmed to deliver background insulin in tiny pulses. These pulses are called basal rates.
When you eat or need a correction, you tell the pump to deliver a larger dose called a bolus. If you want a refresher on how insulin acts in the body, see What Insulin Does and Basal Vs Bolus Insulin. Those concepts matter because a pump is really a different way to deliver insulin, not a different hormone.
What the device includes
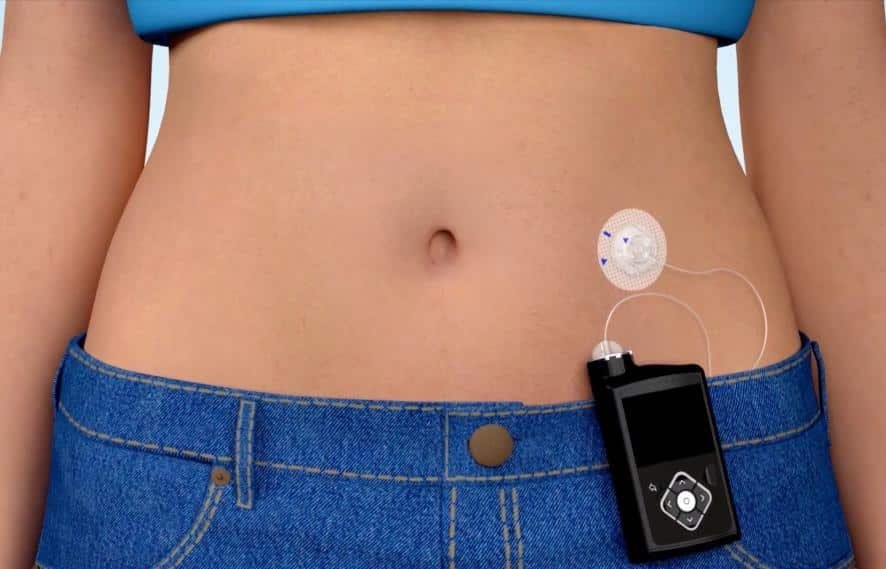
Most systems have a pump body or pod, a reservoir or cartridge, and an infusion set or cannula (a small flexible tube) that sits under the skin. Tubed systems connect the pump to the infusion set. Patch systems place the reservoir and inserter on the body as one unit. The insertion site still needs routine changes and rotation.
Pump therapy typically uses rapid-acting insulin. It does not usually rely on intermediate-acting or premixed insulin products. If insulin types feel confusing, Human Vs Analog Insulin and Lispro Vs Regular Insulin can help frame the differences.
Types of Insulin Pumps
Most insulin pumps fall into three practical groups: tubed pumps, tubeless patch pumps, and automated insulin delivery systems. These categories can overlap. A pump can be tubed and automated, or tubeless and automated.
| Type | How it is worn | What it does well | What to watch |
|---|---|---|---|
| Tubed pump | Pump worn on the body with tubing to an infusion set | Flexible placement, adjustable settings, common option for detailed programming | Tubing management, site changes, visible device attachment |
| Tubeless or patch pump | Pod or patch worn directly on the skin | No external tubing, compact form, simpler wear for some routines | Pod adhesion, fixed wear location, full pod replacement when changed |
| Automated insulin delivery system | Pump paired with a continuous glucose monitor | Can adjust background insulin using sensor data | Still needs user input for meals and attention to alarms or sensor issues |
A continuous glucose monitor, or CGM, measures glucose trends through a sensor worn on the body. When a pump and CGM work together, the system may be called automated insulin delivery or a hybrid closed-loop system. Hybrid is the key word. These systems are not fully hands-off. Many still require meal announcements, carb entry, and regular attention to site problems.
Physical design matters, but daily fit matters more. Some people want no tubing. Others care more about screen controls, data display, button design, charging habits, or how the system works with exercise and sleep. The best choice is usually the one a person can use consistently and troubleshoot confidently.
Who May Use Insulin Pump Therapy
Insulin pump therapy is most common in people with type 1 diabetes, but some people with type 2 diabetes also use it. In general, the question is not only diagnosis. It is also whether the person uses insulin intensively, wants more flexible delivery, and can manage the device safely.
If you want a quick refresher on diabetes terms, T1D And T2D is a helpful starting point. For broader browsing, the Diabetes Hub and Type 1 Diabetes Hub collect related background topics.
Clinicians usually look at several practical factors before recommending a pump:
- Glucose monitoring habits and data review
- Comfort with carb counting or meal estimates
- Ability to respond to alarms and alerts
- Skin tolerance for adhesives and infusion sites
- Hand function, vision, and device handling
- Support at home for children or complex care
Age alone does not decide who can use a pump. Children, teens, adults, and older adults may all use pump therapy. The difference is often training, follow-up, and how much day-to-day support is available. A pump can reduce repeated injections, but it does not remove the need to think about insulin, meals, glucose trends, and sick days.
Benefits, Limits, and Safety Points
The main benefit of an insulin pump is flexible insulin delivery. Basal rates can be adjusted more finely than many injection routines allow. Boluses can be given for meals or corrections without another shot. For some people, that can make daily diabetes management feel more adaptable.
Another advantage is pattern management. Pumps can support different settings at different times of day. That may help people whose insulin needs change overnight, with exercise, or during work and school routines. When paired with a CGM, some systems can reduce or increase background insulin in response to sensor trends.
Still, the limits are real. A pump is worn continuously. Sites need to be changed on schedule. Adhesives can irritate the skin. Tubing can kink. Pods can loosen. Alarms can feel intrusive. The learning curve can also be tiring at first.
Why it matters: Because a pump usually uses only rapid-acting insulin, delivery problems can become urgent faster than many people expect.
That last point is one of the most important safety issues. When insulin delivery stops, there is usually no long-acting insulin in the background. Glucose can rise quickly, and ketones may appear if the problem is not corrected. That is why people using pumps are often taught to watch for unexpected high glucose, check for ketones when advised, and know the warning signs of diabetic ketoacidosis. If you want background on that risk, see Ketosis Vs Ketoacidosis and Ketonuria.
Common pump-related issues include infusion set failure, air in tubing, dislodged sites, empty reservoirs, missed boluses, and insulin that has been exposed to heat or kept too long after opening. None of these problems means pump therapy is a bad option. It means pump therapy works best when the user has a clear troubleshooting routine and a backup way to take insulin if the device fails.
Pump therapy can also change how people think about injections. The number of daily shots usually goes down, but skin care still matters. Site rotation, checking for redness or swelling, and noticing patterns in glucose after site changes are part of safe use.
Starting Insulin Pump Therapy
Starting insulin pump therapy usually involves device selection, hands-on training, initial settings from a clinician, and a plan for meals, exercise, sick days, and device failure. Good starts are rarely fast starts. The first weeks are often about learning patterns, not chasing perfect numbers.
Training often covers how to fill the reservoir or activate the pod, insert the cannula, program basal and bolus settings, and use correction features. Many people also learn how the pump works with a CGM, how to read trend arrows, and when not to rely on automation alone.
Helpful questions to ask before starting include:
- Training plan: who teaches setup and site changes
- Insulin choice: which rapid-acting insulin the system uses
- Backup method: pens or syringes if the pump stops
- CGM fit: which sensors work with the device
- Sick-day plan: when to check ketones and call for help
- Supply routine: how often sets, pods, or cartridges change
- Data review: how settings are adjusted after startup
People often focus on the device and forget the backup plan. That is a mistake. Pumps can fail, fall off, or alarm at inconvenient times. A written plan for missed insulin, persistent high readings, and after-hours problems matters just as much as the pump itself.
Site placement is another practical issue. Pump infusion sites are not exactly the same as injection sites, but the same basic idea applies: use healthy tissue, rotate locations, and avoid overusing one spot. For general site-rotation basics, Where To Inject Insulin is useful background.
Prescription details may need confirmation with the prescriber.
Day-to-Day Use and Common Troubleshooting
Daily pump use centers on three habits: checking glucose data, keeping the device supplied, and reacting early when something looks off. Most problems are easier to fix when they are caught early.
A practical daily review may include insulin remaining, battery or charge status, pump or pod adhesion, site age, CGM trend direction, and whether recent boluses were actually delivered. These checks take little time, but they prevent avoidable surprises.
If glucose is higher than expected and not coming down, common things to check include a loose site, bent cannula, occlusion alarm, empty reservoir, expired pod wear time, missed meal bolus, or insulin that may no longer be working well. Persistent high readings with nausea, vomiting, or ketones are more serious and should not be ignored.
Quick tip: Keep backup insulin, supplies, and ketone-testing materials with your routine gear.
Travel, sports, swimming, sleep, and work all add small practical questions. Can the device stay connected? Does the site stay secure with sweat? Will alarms disturb meetings or sleep? These details often matter more than headline features. A device that looks appealing on paper may still be a poor fit if the daily routine does not match.
Where permitted, licensed third-party pharmacies handle dispensing and fulfilment.
Access and Cost Context
Access to pump therapy usually depends on a prescription, device training, ongoing supplies, and coverage rules that vary by plan and region. The cost question is not just the pump itself. It also includes infusion sets or pods, cartridges or reservoirs, adhesives, and sometimes a CGM if the system depends on one.
Coverage can differ widely between employers, public programs, and private insurance plans. Some plans cover the device but not all monthly supplies. Others require specific paperwork or proof of medical need. Because of that, the best practical step is often to ask for a full list of covered items, refill rules, and replacement policies before choosing a system.
Some people also explore cash-pay options when coverage is limited. That can be reasonable, but the details depend on eligibility, local rules, and the exact device or supply. It helps to compare the ongoing monthly pieces, not only the first purchase.
For readers who want broader background before looking at devices or supplies, the Diabetes Condition Hub and Type 1 Diabetes Condition Hub offer browseable condition-based starting points.
Further Reading
An insulin pump can make insulin delivery more flexible, but it is not automatic in the everyday sense. The core skills still matter: understanding basal and bolus insulin, rotating sites, watching for unexplained highs, and keeping a backup plan.
Cash-pay or cross-border options depend on eligibility and jurisdiction.
If you still feel unsure, the next useful step is not more jargon. It is a focused conversation about training, supplies, CGM compatibility, and what you would do if the device stopped delivering insulin.
Authoritative Sources
- American Diabetes Association consumer overview of insulin pumps
- Cleveland Clinic overview of insulin pump basics and types
- Peer-reviewed clinical overview of insulin pump therapy
This content is for informational purposes only and is not a substitute for professional medical advice.

{kind=link}
{kind=link}