
Insulin vs glucagon is a comparison of two pancreatic hormones with opposite jobs: insulin lowers blood glucose, while glucagon raises it when levels fall. This balance matters because the brain needs a steady glucose supply, but sustained high glucose can also harm the body. For people using diabetes medications, the difference also helps explain meals, fasting, exercise, hypoglycemia, and emergency glucagon use.
Key Takeaways
- Opposite effects: insulin lowers glucose, while glucagon raises it.
- Shared goal: both hormones help keep blood glucose within a safer range.
- Pancreas source: beta cells release insulin, and alpha cells release glucagon.
- Emergency role: glucagon can treat severe hypoglycemia when swallowing is unsafe.
- Planning helps: train helpers, check supplies, and monitor after recovery.
How Insulin and Glucagon Work Together
Insulin and glucagon work as a paired control system for blood glucose. After a meal, glucose enters the bloodstream and insulin helps move it into cells. Between meals, during overnight fasting, or after prolonged activity, glucagon signals the liver to release stored glucose.
This push-pull relationship is sometimes compared with a thermostat. Insulin turns down glucose when levels rise. Glucagon turns glucose back up when levels fall. The goal is not for one hormone to “win,” but for both to respond at the right time.
The pancreas produces both hormones, but different cell types handle each one. Pancreatic beta cells make insulin. Pancreatic alpha cells make glucagon. These cells sit in clusters called islets, where they can respond quickly to changes in blood glucose and other metabolic signals.
For a deeper companion explainer on the shared hormone system, see Insulin Glucagon. That page expands on how the two hormones coordinate energy use across the liver, muscle, and fat tissue.
Why it matters: Knowing which hormone raises or lowers glucose can make diabetes education clearer during meals, exercise, illness, and emergencies.
Insulin Function: How It Lowers Blood Sugar
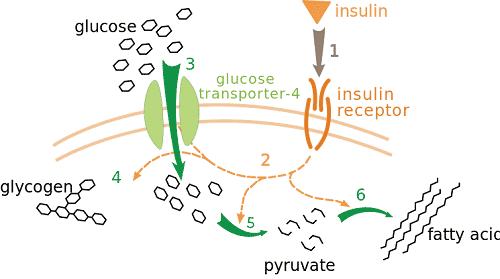
Insulin lowers blood sugar by helping glucose leave the bloodstream and enter body tissues. Muscle and fat cells respond to insulin by moving glucose transporters to the cell surface. This allows more glucose to move into cells, where it can be used for energy or stored for later.
The liver also responds strongly to insulin. When insulin levels rise, the liver stores glucose as glycogen, a storage form of glucose. Insulin also helps reduce the liver’s own glucose production. Together, these actions slow the rise in blood glucose after meals.
Insulin has broader metabolic effects as well. It supports glycogen storage in muscle, reduces fat breakdown, and helps shift the body toward nutrient storage after eating. These effects are normal parts of metabolism, not only diabetes treatment.
In diabetes care, prescribed insulin products try to replace or supplement this natural insulin pattern. Some insulins are designed to work around meals. Others provide background coverage between meals and overnight. If you want more detail on the molecule itself, Insulin Chemical Structure explains insulin’s protein structure in plain language.
Some readers also want to understand why insulin products are not interchangeable without professional guidance. The overview Insulin Products Guide explains how onset, duration, formulation, and device factors can differ.
Glucagon Function: How It Raises Blood Sugar
Glucagon raises blood sugar mainly by acting on the liver. When blood glucose falls, glucagon signals the liver to break down glycogen and release glucose into the bloodstream. It can also support gluconeogenesis, which means making new glucose from non-carbohydrate sources.
This response helps protect the brain during fasting or low glucose. The brain depends heavily on a steady fuel supply. When glucose drops too far, symptoms may include shakiness, sweating, confusion, weakness, seizure, or loss of consciousness.
Glucagon is a hormone, not a sugar and not a stored fuel. A common mix-up is glucagon vs glycogen. Glucagon is the signal. Glycogen is the stored glucose reserve, mainly in the liver and muscle. In simple terms, glucagon tells the liver to use glycogen when blood glucose needs support.
The glucagon and insulin relationship also changes during exercise, illness, and missed meals. For example, activity can increase glucose use by muscle. If insulin levels are still active and carbohydrate intake is low, glucose may fall. Glucagon helps counter that drop, but the response may not always be enough, especially in some people with long-standing diabetes.
Insulin vs Glucagon at a Glance
The simplest difference is direction: insulin moves glucose out of the blood, while glucagon moves glucose into the blood. The details below show how their timing, source, and main targets differ.
| Feature | Insulin | Glucagon |
|---|---|---|
| Main effect | Lowers blood glucose | Raises blood glucose |
| Released by | Pancreatic beta cells | Pancreatic alpha cells |
| Common trigger | Rising glucose after eating | Falling glucose during fasting or lows |
| Main liver action | Promotes glucose storage as glycogen | Promotes glycogen breakdown and glucose release |
| Key tissue targets | Liver, muscle, and fat tissue | Mainly the liver |
| Diabetes context | May be prescribed to treat hyperglycemia | May be used for severe hypoglycemia emergencies |
This table is useful for orientation, but real physiology is more complex. Other hormones, food composition, stress, sleep, medications, and physical activity also affect glucose levels. That is why repeated highs or lows should be reviewed with a healthcare professional rather than managed by guesswork.
If you track glucose in different units, a conversion tool can reduce confusion when reading labels, logs, or international resources. It only converts values and does not interpret whether a reading is safe for you.
Blood Glucose Unit Converter
Convert glucose readings between mg/dL and mmol/L without changing the clinical value.
These calculations are for education only and do not replace clinical advice, diagnosis, or treatment. Always confirm medical decisions with a qualified healthcare professional.
Emergency Glucagon: When It May Be Used
Emergency glucagon is used for severe hypoglycemia when a person cannot safely self-treat with fast-acting carbohydrate. Examples include unconsciousness, seizure, extreme confusion, or inability to swallow. In these situations, a trained helper should give glucagon according to the product instructions and activate emergency services.
Do not give food or drink to someone who is unconscious or cannot swallow. This can cause choking or aspiration, which means fluid or food entering the airway. Positioning the person on their side may help reduce this risk while waiting for emergency help.
Several glucagon products exist. Some kits require mixing a powder with liquid before injection. Other products may be ready to use or given through the nose. The best emergency plan is the one that caregivers can find, understand, and use under stress.
For a practical walkthrough of a traditional kit, see Use Glucagon Injection Kit. Product-specific instructions still matter, so check the device you actually keep at home, work, school, or in a travel bag.
People comparing emergency options may also review product pages for device familiarity. Examples include Glucagon Injection Kit and Baqsimi Nasal Powder. These pages should not replace instructions from a clinician, pharmacist, or the product label.
What Helpers Should Know Before a Low Happens
Training works best before an emergency. Helpers should know where glucagon is stored, when to use it, how to follow the device instructions, and when to call emergency services. They should also know not to give oral carbohydrate until the person is awake and can swallow safely.
- Find the kit: store it where helpers can access it quickly.
- Check dates: replace expired supplies before they are needed.
- Review instructions: practice with trainer materials if available.
- Assign roles: one person treats while another calls for help.
- Monitor after: keep watching because glucose may fall again.
For non-severe lows, oral carbohydrate may be appropriate when the person is awake and able to swallow. The article Low Blood Sugar Steps explains general hypoglycemia response concepts for less severe situations.
Monitoring After Glucagon or a Low
Monitoring after a low helps confirm recovery and detect another drop. Glucagon can raise glucose, but the underlying cause may still be present. Active insulin, missed food, vomiting, alcohol use, or prolonged activity can all increase the chance of another low.
Once the person is awake and can swallow, follow the care plan provided by their healthcare team. Many plans include checking glucose again and using food or drink to help maintain glucose. If symptoms persist, glucose remains low, or the person does not recover as expected, emergency care is needed.
Continuous glucose monitors can be helpful, but fingerstick checks may still be needed in urgent situations. Sensor readings can lag behind blood glucose during rapid changes. This is especially relevant after treatment for hypoglycemia, when glucose may be rising quickly.
Quick tip: Keep emergency instructions with the glucagon device, not only in a phone.
Where Diabetes Treatment Fits Into the Hormone Balance
Diabetes can disrupt the normal insulin and glucagon balance in different ways. In type 1 diabetes, the body makes little or no insulin. In type 2 diabetes, insulin resistance often means cells respond less effectively to insulin, and insulin production may decline over time.
Insulin treatment may be used when the body does not make enough insulin or when other therapies are not enough. Examples of insulin product pages include Humalog Vial, Lantus Vial, and Novolin ge Toronto Vial. These examples differ in clinical use and timing, so treatment decisions should come from a licensed healthcare professional.
Glucagon planning is often part of safety education for people at risk of severe hypoglycemia. Risk can vary based on insulin use, meal timing, activity, kidney function, alcohol intake, past severe lows, and awareness of symptoms. A clinician can help decide whether emergency glucagon belongs in a specific care plan.
CanadianInsulin.com provides educational content and product navigation as a prescription referral platform. Where required, prescription details may be confirmed with the prescriber, while dispensing is handled by licensed third-party pharmacies where permitted.
Food, Low Blood Sugar, and Common Misunderstandings
Food choices can affect glucose, but no single food is universally the “worst” or “best” for every person with diabetes. Portion size, carbohydrate amount, fiber, fat, protein, medication timing, and personal glucose response all matter. This is why broad food rankings can mislead people.
Nuts and peanut butter are common examples. Nuts can fit many eating patterns, but sweet coatings, large portions, or added sugars can change their glucose impact. Peanut butter contains fat and protein, so it may slow digestion. It is not usually the fastest option for treating an urgent low because severe hypoglycemia requires rapid carbohydrate or emergency care, depending on the situation.
For mild lows when a person is awake and able to swallow, many care plans use fast-acting carbohydrate first. Longer-acting food may come later, depending on the plan and timing of the next meal. People with recurrent lows, pregnancy, kidney disease, gastroparesis, eating disorders, or medication-related hypoglycemia should discuss carbohydrate targets with a clinician or registered dietitian.
For broader browsing, the Diabetes Articles collection gathers related educational topics. The Diabetes Condition page and Diabetes Products category provide navigation to relevant listings.
Authoritative Sources
For patient-oriented background on glucagon and its role in raising glucose, see the Cleveland Clinic glucagon overview.
For emergency hypoglycemia recommendations and standards used in diabetes care, review the American Diabetes Association Standards of Care.
For regulatory information on approved drug labels, search the FDA Drugs@FDA database by product name.
Recap
Insulin vs glucagon comes down to direction and timing. Insulin helps lower glucose after meals and supports storage. Glucagon helps raise glucose during fasting or severe lows by signaling the liver to release glucose. Both hormones are essential parts of glucose regulation.
For people managing diabetes, the practical message is preparation. Know the signs of hypoglycemia, keep monitoring tools available, teach helpers how to respond, and review repeated lows or severe events with a healthcare professional. In suspected severe hypoglycemia, activate emergency services and follow local emergency instructions while using glucagon if it is part of the plan.
This content is for informational purposes only and is not a substitute for professional medical advice.


{kind=link}
{kind=link}