
An artificial pancreas is an automated insulin delivery system that links a continuous glucose monitor, an insulin pump, and control software. It does not replace the pancreas as an organ. Instead, it adjusts insulin delivery in response to glucose trends, which may reduce daily decision burden for some people using intensive insulin therapy.
Recent studies in adults with type 2 diabetes suggest these systems can improve glucose control in selected patients. The strongest evidence still comes from type 1 diabetes care, but research in type 2 diabetes is expanding. Why this matters is simple: automated dosing may help people spend more time in range while still requiring training, supplies, and a backup plan.
Key Takeaways
- Closed-loop systems use CGM data to adjust insulin delivery.
- They support insulin treatment but do not cure diabetes.
- Type 2 diabetes trials show promise in selected adults.
- Device wear, alarms, and supply costs remain important limits.
- Access depends on approvals, coverage rules, and clinic support.
What an Artificial Pancreas Does
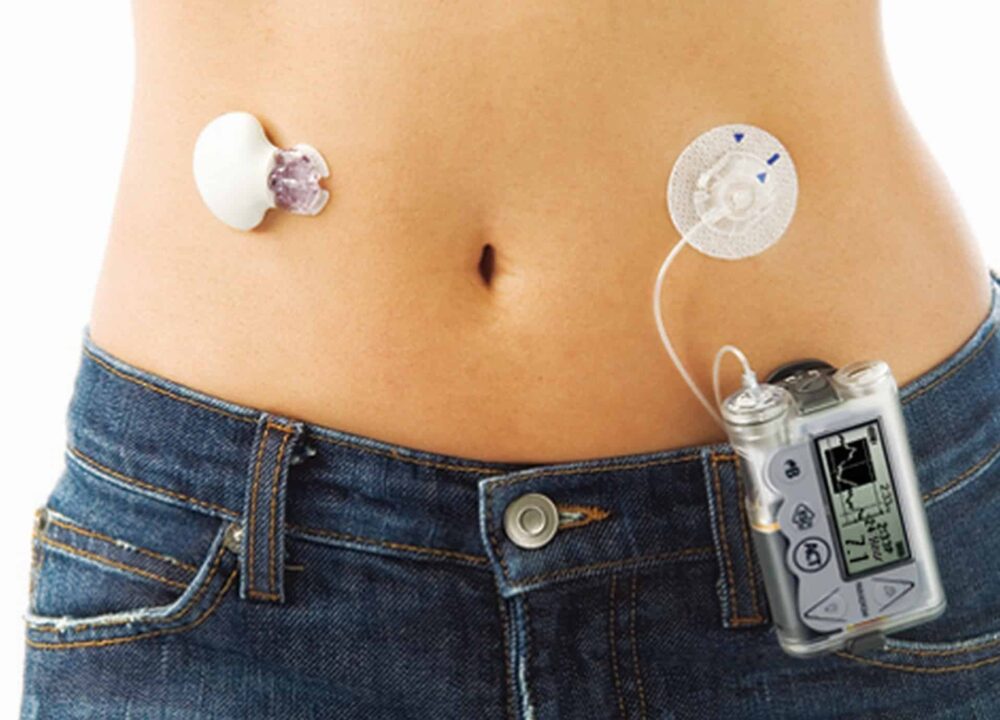
An artificial pancreas works by creating a feedback loop between glucose readings and insulin delivery. A continuous glucose monitor, or CGM, checks glucose levels under the skin every few minutes. An insulin pump delivers rapid-acting insulin through an infusion set. The algorithm uses recent readings and glucose trends to increase, reduce, or pause insulin delivery within programmed safety limits.
This design is often called automated insulin delivery or closed-loop insulin delivery. Some systems are hybrid closed-loop systems because users still enter meal information, confirm prompts, or adjust settings with their care team. Other systems aim to reduce carbohydrate counting and rely more heavily on adaptive dosing.
The system can respond more often than a person can reasonably calculate insulin needs. That is the main advantage. It may smooth out overnight glucose swings, respond to rising glucose after meals, and reduce some repetitive corrections. Still, it cannot detect every situation. Infusion set problems, sensor errors, missed meal inputs, illness, and exercise can still affect glucose control.
For a broader look at the devices that support automated care, see Diabetes Tech. For CGM-specific background, Continuous Glucose Monitoring explains how sensor readings fit into daily diabetes management.
Why Trials in Type 2 Diabetes Matter
Trials in type 2 diabetes matter because many adults with type 2 diabetes eventually use complex insulin regimens. Basal-bolus insulin therapy can require multiple daily decisions about meals, corrections, activity, and overnight glucose patterns. Automation may reduce some of that work, especially for people already using intensive insulin treatment.
In clinical studies, researchers often track time in range, mean glucose, A1C, hypoglycemia, and device use. Time in range means the percentage of time glucose stays within a target band set by the care team. It can show daily glucose stability in a way that a single A1C value cannot. Some studies of closed-loop technology in type 2 diabetes have reported better time in range and fewer overnight lows, although results vary by population and study design.
The artificial pancreas for type 2 diabetes is not a universal next step for every person with the condition. It is most relevant when insulin treatment is already intensive, glucose patterns are difficult to manage, or hypoglycemia risk is a recurring concern. People using simpler medication plans may not need pump-based automation.
Why it matters: Trial results help clinicians decide where automation adds practical value.
If you are comparing glucose numbers over time, a time-in-range estimate can help organize CGM data before a clinical review. It does not replace professional interpretation.
CGM Time-in-Range Summary
Summarise CGM percentages across very low, low, in-range, high, and very high glucose bands.
These calculations are for education only and do not replace clinical advice, diagnosis, or treatment. Always confirm medical decisions with a qualified healthcare professional.
How the System Compares With Standard Pump Therapy
The key difference between an artificial pancreas and a standard insulin pump is automation. A conventional pump delivers basal insulin and boluses based on programmed settings and user inputs. An automated system uses CGM trends to adjust insulin delivery more frequently, within safety boundaries.
Many readers compare a bionic pancreas vs insulin pump because both involve wearable hardware. The practical difference is how much decision-making stays with the user. Traditional pump users often manage basal rates, carbohydrate ratios, correction factors, and meal boluses more directly. Bionic or automated systems may reduce some of those decisions, depending on the model and settings.
Comparisons such as iLet Bionic Pancreas vs Tandem insulin pump or iLet Bionic Pancreas vs Omnipod 5 usually come down to workflow, not one simple winner. People often consider whether they prefer tubed or tubeless wear, how meal announcements work, how much manual control they want, and which CGM sensors are compatible. These details can change over time, so device labeling and clinic guidance matter.
It also helps to compare the system with daily fingerstick and insulin routines. A person who uses multiple daily injections may see the biggest change in wear burden, device training, and supply management. Someone already using a pump may notice more change in software behavior and alarm handling than in the physical routine.
For glucose targets and common measurement terms, Blood Sugar Ranges offers useful context. For monitoring frequency and daily testing questions, see Blood Sugar Monitoring.
iLet Bionic Pancreas and Daily Use Questions
The iLet Bionic Pancreas is one example of an automated insulin delivery system. In general terms, it is designed to simplify some dosing decisions compared with conventional pump therapy. Users may still need to wear a sensor, manage infusion sites, respond to alarms, and follow training instructions.
People often ask how does the iLet Bionic Pancreas work. Its workflow is built around system learning and simplified meal handling, rather than traditional detailed pump programming. However, any specific device should be understood through its current instructions for use, approved indication, compatible supplies, and clinician training materials.
Reader interest in iLet Bionic Pancreas reviews is understandable, but personal reviews have limits. A review may reflect one person’s skin tolerance, alarm preferences, insurance coverage, or glucose variability. Structured clinical data and post-market safety information are more useful for understanding overall performance. Personal reports can still help identify practical questions to ask before starting.
Daily tasks still matter
Automation does not remove basic device care. Users still need to change sensors and infusion sets as directed, rotate sites, charge or replace components when needed, and check alerts. They also need a plan for sensor downtime, pump failure, or persistent high glucose. Care teams usually review backup insulin instructions before someone depends on pump-based delivery.
Meal and exercise patterns still matter
Meals, exercise, alcohol, illness, stress, and sleep can all shift insulin needs. Automated systems react to glucose trends, but they may not always prevent a rise or low in advance. This is why training focuses on alarms, trend arrows, site checks, and when to confirm readings with a fingerstick meter.
For a general primer on insulin needs and dose concepts, Insulin Dosage Concepts explains why dosing decisions require clinical oversight.
Access, Availability, and Cost Factors
Access to an artificial pancreas depends on the country, device approval, insurance rules, and whether local clinics can train users safely. Availability is not just a question of whether a device exists. It also depends on compatible sensors, pump supplies, software support, and prescriber familiarity.
Questions such as when will artificial pancreas be available or when will the iLet Bionic Pancreas be available do not have one global answer. Regulatory approval, payer coverage, and launch plans vary by region. A system may be approved for one diabetes population before another. It may also be available through some clinics or plans before broader access expands.
Cost discussions should include more than the pump itself. The bionic pancreas cost or artificial pancreas price may involve sensors, transmitters, infusion sets, reservoirs, training visits, replacement parts, and follow-up support. Insurance may cover some items differently, and prior authorization can be required. People without stable coverage may face different choices than those with durable medical equipment benefits.
CanadianInsulin.com is a prescription referral platform, and device-related access questions can involve documentation from a prescriber when required. Dispensing and fulfilment, where permitted, are handled by licensed third-party pharmacies rather than by the editorial content itself. Some patients also explore cash-pay options depending on eligibility and jurisdiction.
The most useful next step is usually a focused discussion with a diabetes clinician. Ask which systems are approved for your situation, which supplies are covered, what training is required, and what backup plan is needed if automation stops.
Benefits, Limits, and Safety Considerations
The main potential benefits are better time in range, fewer glucose swings, less overnight worry, and fewer manual insulin decisions. These benefits are not guaranteed. They depend on the user’s insulin needs, device setup, wear time, support, and ability to respond to alerts.
The disadvantages of artificial pancreas systems are also practical. Some people dislike wearing devices continuously. Adhesive irritation can occur. Alarms may interrupt sleep or work. Sensor failures, infusion set occlusions, or connectivity problems can affect insulin delivery. These issues are manageable for many users, but they require preparation.
Safety planning should cover both low and high glucose. A system may reduce insulin when glucose is falling, but it cannot make food appear or treat severe hypoglycemia. It may increase insulin when glucose rises, but it cannot fix a kinked infusion set or a failed sensor. Users should know when to check ketones, when to use backup insulin, and when to seek urgent medical care, based on their care plan.
Quick tip: Keep backup supplies separate from your everyday device bag.
People should seek urgent care for severe hypoglycemia, confusion, loss of consciousness, repeated vomiting, signs of diabetic ketoacidosis, or very high glucose that does not improve according to their sick-day plan. These situations need medical assessment and should not be managed by device settings alone.
Questions to Ask Before Starting
A structured conversation can help match the technology to the person, not just the diagnosis. The goal is to understand how the system will fit daily life, work, sleep, meals, travel, and medical follow-up.
- Eligibility: Ask whether the device is approved for your diabetes type and insulin regimen.
- Training: Confirm who teaches setup, alarms, site changes, and troubleshooting.
- Supplies: Review sensors, infusion sets, reservoirs, and replacement schedules.
- Backup plan: Ask what to do if the pump, sensor, or algorithm fails.
- Coverage: Check which components are covered separately or together.
- Data review: Ask how often the care team reviews CGM and pump reports.
- Lifestyle fit: Discuss shift work, exercise, travel, alcohol, and skin sensitivity.
People with pregnancy, kidney disease, gastroparesis, recurrent severe lows, eating disorders, or frequent diabetic ketoacidosis should discuss technology choices carefully with a specialist. These situations can change glucose patterns and safety planning.
For condition-specific browsing, the Type 2 Diabetes Collection groups related educational posts. The Type 2 Diabetes Products page can also help readers understand how treatment categories are organized on the site.
Authoritative Sources
For a regulator’s definition and safety framing, the FDA explains what an artificial pancreas device system is. This resource clarifies that the system mimics glucose regulation through linked devices rather than replacing the organ.
For patient-oriented background from a major health agency, the NIDDK provides an overview of artificial pancreas systems. It covers the three main components and how they work together.
For broader standards on diabetes technology, the American Diabetes Association publishes annual Standards of Care updates. These statements summarize evidence and clinical considerations for CGM, pumps, and automated insulin delivery.
Recap
An artificial pancreas can help automate insulin delivery by connecting CGM readings, pump delivery, and control software. Trials in type 2 diabetes are encouraging for selected adults using intensive insulin therapy, but access and suitability vary. The best decision depends on clinical history, training support, coverage, device preferences, and a clear backup plan.
This content is for informational purposes only and is not a substitute for professional medical advice.

{kind=link}
{kind=link}