
How much is insulin without insurance depends on the insulin type, your monthly dose, the device, and the pharmacy quote. In 2025, many U.S. cash-pay patients may find lower posted costs than in past years because of manufacturer list-price cuts, assistance programs, and retail human insulin options. Still, the amount due at the counter can vary widely, especially for analog pens, basal insulin, or mixed regimens.
Why this matters: insulin is not optional for many people with diabetes. A cost change can affect refill timing, device choice, and conversations with your prescriber. This guide explains the main cost drivers, what changed recently, and how to compare options without making unsafe therapy changes.
Key Takeaways
- Product type matters: analogs, biosimilars, and human insulin often differ.
- Monthly dose matters: more units usually means more vials or pens.
- Pharmacy quotes vary: cash, assistance, and 90-day totals can differ.
- Insurance rules matter: deductibles, tiers, and caps change your share.
- Switching needs review: timing and glucose effects may change.
Current Cash-Pay Ranges and Why They Vary
The simplest answer is that a 30-day insulin supply can range from relatively low-cost human insulin at some large retailers to much higher totals for some analog pens or multiple-insulin regimens. The final amount depends on the exact product, the number of units used each day, and whether you use vials, prefilled pens, or cartridges.
Human regular insulin and NPH insulin are older formulations. They may have lower retail cash options in many areas, but they work differently from rapid-acting or long-acting analogs. Rapid-acting analogs are often used around meals. Long-acting basal insulin is often used to provide background coverage. Those timing differences matter clinically, so cost alone should not drive a switch.
Device format also changes the total. Vials may cost less per unit, but they require syringes and careful measuring. Pens can be easier for some people, but they may cost more and can create waste if partial pens expire or are discarded. If you are comparing long-acting options, Tresiba vs Lantus explains how basal insulins are commonly discussed in care plans.
Pharmacies do not always show the same cash quote. A national chain, independent pharmacy, clinic pharmacy, and mail-order service may list different totals. The quote can also change if a pharmacy applies a manufacturer program, a savings arrangement, or a cash-pay card. Ask for the full amount due, the package size, and the units supplied so you can compare the same quantity.
How Many Vials or Pens You May Need Each Month
Your monthly quantity depends on your prescribed total daily insulin units. Someone using a small basal-only dose may need fewer packages than someone using basal and mealtime insulin. People using insulin pumps may have different supply patterns because they also need pump supplies and infusion sets.
A useful comparison starts with units, not boxes. For example, one person may compare the cost per 1,000 units in a vial with the cost per 1,500 or 3,000 units in a pen package, depending on how the product is packaged. You do not need to change your dose for this math. You are only comparing what you already use against the package amount supplied.
Blood Glucose Unit Converter
Convert glucose readings between mg/dL and mmol/L without changing the clinical value.
These calculations are for education only and do not replace clinical advice, diagnosis, or treatment. Always confirm medical decisions with a qualified healthcare professional.
This converter helps with blood glucose unit conversion between mg/dL and mmol/L. It is included for readers comparing records from different systems or international sources, not to change insulin dosing.
Waste can affect monthly cost. Pens and vials have use-after-opening limits that depend on the product label. If a package expires before you use it, the practical cost per unit rises. Your pharmacist can confirm storage and in-use instructions from the product label.
Quick tip: Ask the pharmacist to quote the same prescription as a 30-day and 90-day fill, then compare total units supplied.
Why the U.S. Insulin Bill Can Look Different With Insurance
Insurance changes the patient share, but it does not always make the first fill cheaper. Deductibles, coinsurance, copays, formulary tiers, and preferred brands determine what you pay. During a deductible phase, a plan member may temporarily see an amount that feels close to a cash quote. After the deductible, the share may drop.
Medicare has a clearer rule for many beneficiaries. Under current federal policy, covered insulin under Medicare Part D and certain insulin used with durable medical equipment under Part B are capped monthly. The details depend on coverage type and whether the product is covered by the plan or supplier. The Medicare insulin coverage page summarizes the current federal cap.
Commercial insurance is less uniform. Some employer and marketplace plans have copay caps, preferred insulin lists, or special programs. Others may require prior authorization or step therapy for certain brands. If your insulin changed tiers this year, ask the plan for the formulary reason and whether a clinically appropriate alternative is preferred.
People also ask who qualifies for $35 insulin. Medicare beneficiaries often qualify for the federal monthly cap when the insulin is covered under the relevant Medicare benefit. Some manufacturer programs may also reduce costs for eligible uninsured or commercially insured patients, but criteria differ. The American Diabetes Association affordability resource outlines common assistance pathways.
Human Insulin, Analogs, and Biosimilars
The cheapest insulin without insurance is often an older human insulin option, but “cheapest” does not mean interchangeable for every regimen. Regular insulin, NPH insulin, rapid-acting analogs, long-acting analogs, and premixed products have different onset, peak, and duration patterns. Those differences can affect meal timing, overnight glucose, and hypoglycemia risk.
Analog insulin is modified to change how it behaves after injection. Many people use rapid-acting analogs for meals and long-acting analogs for background coverage. Biosimilar or follow-on versions may create lower-cost alternatives in some categories, although pharmacy substitution rules and plan coverage vary by state and product.
If your prescriber mentions insulin alternatives, ask whether the change is therapeutic, administrative, or cost-related. A formulary switch may be reasonable for some people, but it still requires clear instructions. For background on one common alternative discussion, Basaglar Generic Name explains how naming and alternatives can become confusing.
Some readers compare specific product formats while reviewing options. Browseable diabetes product collections, such as the Diabetes Product Category, can help you see examples of available formats. Product pages should not replace advice from your prescriber or pharmacist.
Why Insulin Has Been So Expensive in the U.S.
The U.S. insulin price problem comes from several layers, not one single cause. List prices, pharmacy benefit manager rebates, plan formularies, pharmacy markups, patent and device strategies, and limited competition have all affected what patients see at the counter.
List price is the public starting amount set by a manufacturer. Net price is what a payer may spend after rebates and contracts. A cash-paying patient may not benefit from negotiated rebates, so the list-to-net gap can matter. This is one reason two people using the same insulin can report very different out-of-pocket costs.
The cost of insulin production is only one part of the final price. Manufacturing sterile injectable medicines requires quality controls, packaging, storage, distribution, and regulatory compliance. Even so, public debate often focuses on why established insulin products remained costly after decades of use. The answer usually involves both production complexity and the structure of U.S. drug payment.
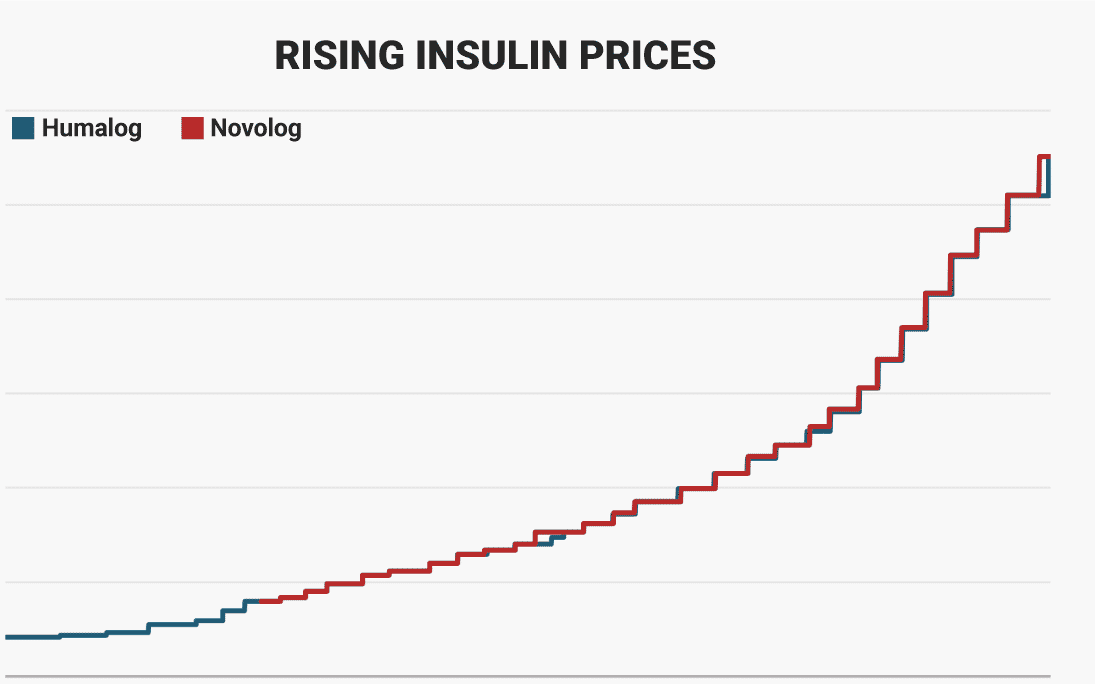
The price of insulin over the last 10 years has not moved in one straight line. Many list prices rose sharply during the prior decade. Then, several major manufacturers announced list-price reductions and affordability programs in 2023 and later. Real-world prices in 2024 and 2025 depend on whether pharmacies, plans, and manufacturers applied those changes to the specific insulin being filled.
How U.S. Costs Compare With Other Countries
Insulin price USA comparisons often look high because the U.S. payment system is fragmented. Other countries may use national negotiation, reference pricing, public formularies, or tighter limits on markups. Those systems can lower official or negotiated prices, but they are not identical to U.S. retail pharmacy conditions.
Canada is a common comparison for U.S. readers. The gap can reflect negotiated pricing, provincial coverage rules, and different supply-chain incentives. Some patients explore cash-pay options and cross-border fulfilment depending on eligibility and jurisdiction. Where required, prescription details may need confirmation with the prescriber, and dispensing is handled by licensed third-party pharmacies where permitted.
International comparisons can help explain market structure, but they do not tell you which insulin to use. Product names, package sizes, labels, and substitution rules can differ by country. If you are reviewing diabetes-related options broadly, the Diabetes Condition Collection provides a browseable starting point.
Practical Ways to Compare Costs Safely
The safest cost comparison starts with your current prescription and clear questions. Do not ration insulin or stretch doses to lower spending. If your refill is unaffordable, contact your prescriber, pharmacist, insurer, or an emergency assistance resource as soon as possible.
- Confirm the product: brand, generic name, concentration, and device.
- Calculate monthly units: use prescribed daily units only.
- Compare package totals: vials and pens may contain different units.
- Ask about alternatives: request clinically appropriate options only.
- Check assistance rules: eligibility can vary by coverage and income.
- Review supplies: syringes, pen needles, and glucose supplies add cost.
- Plan refills early: urgent fills can limit comparison time.
Low-income programs may help when routine pharmacy costs become unmanageable. Low-Income Medication Options reviews practical categories of support that people commonly explore. If your prescription is for a specific mealtime insulin format, Humalog Cartridge Refills offers a related discussion about refill planning and device-related costs.
State rules can also matter. Some states have insulin copay caps for certain insurance plans, while others provide emergency access programs. These rules may not apply to every plan type, especially self-funded employer plans. For a broader policy view, State-by-State Insulin Pricing explains how local rules can differ.
Why it matters: a lower monthly bill is only helpful if the insulin still matches your prescribed regimen.
When Cost Problems Become a Safety Issue
Cost becomes a medical safety issue when it leads to missed doses, rationing, skipped meals, or repeated high or low blood glucose readings. Seek urgent medical care for severe hypoglycemia, confusion, fainting, vomiting with high glucose, ketones, or symptoms of diabetic ketoacidosis. These situations can become dangerous quickly.
Tell your care team if you are stretching insulin or supplies. A prescriber may be able to document medical necessity, request a formulary exception, change to a covered option, or connect you with assistance. A pharmacist can help identify whether the issue is a deductible, non-preferred product, package size, or missing assistance program.
Caregivers should also know where insulin, glucagon, meters, continuous glucose monitoring supplies, and emergency contacts are stored. Cost conversations often focus on the insulin itself, but safety planning includes supplies and clear instructions. If a device or brand is changed, ask for teaching before the first fill whenever possible.
Authoritative Sources
For current federal coverage rules, review the Medicare insulin coverage page.
For assistance pathways and affordability resources, see the American Diabetes Association insulin resource.
For background on biosimilars and interchangeable products, the FDA biosimilars information hub explains regulatory concepts.
Bottom Line
How much is insulin without insurance is a practical question, but there is no single national answer. The amount depends on the insulin, device, monthly units, pharmacy quote, assistance eligibility, and whether older human insulin is clinically appropriate. Recent list-price reductions and federal caps have changed the landscape, but local pharmacy and plan details still matter.
Use unit-based comparisons, ask for multiple pharmacy quotes, and involve your prescriber before changing products. If costs threaten your ability to take insulin as prescribed, treat that as a medical access problem, not a budgeting issue alone.
This content is for informational purposes only and is not a substitute for professional medical advice.

{kind=link}
{kind=link}