
An insulinoma is a rare pancreatic neuroendocrine tumor that releases insulin when the body does not need it. That excess insulin can cause repeated low blood sugar, especially during fasting, overnight, or after exercise. Symptoms may start with sweating, shaking, hunger, or palpitations, but more severe episodes can bring confusion, blurred vision, seizures, or fainting. Diagnosis usually combines symptoms during low glucose, blood tests obtained during a supervised fast, and imaging to locate the tumor. Treatment often centers on surgery, with other options used when surgery is not possible or disease is more complex.
Key Takeaways
- Rare beta-cell tumor that can trigger endogenous hyperinsulinemic hypoglycemia.
- Symptoms usually reflect low blood sugar, not pain from the pancreas.
- Whipple triad helps frame the diagnosis.
- A supervised fast and paired blood tests are often central to the workup.
- Surgery is the main treatment for localized disease, but follow-up still matters.
What Insulinoma Is and Why Symptoms Happen
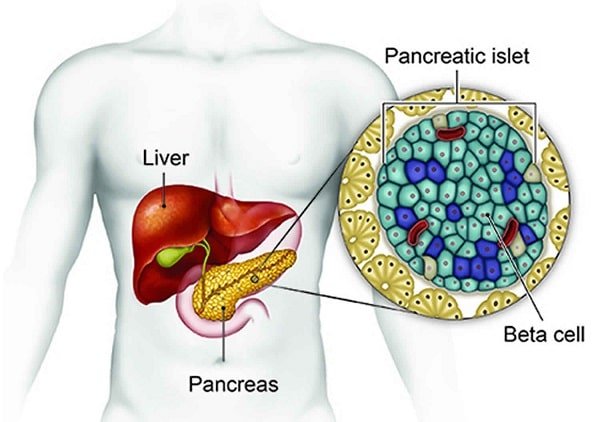
This tumor starts in the pancreatic beta cells, the cells that normally release insulin after meals. In plain language, it is a beta-cell tumor of the pancreas. In this setting, insulin secretion can continue even when glucose is already low. That creates endogenous hyperinsulinemic hypoglycemia, meaning the body itself is making too much insulin and pushing blood sugar down.
That mechanism is different from the patterns described in Insulin Resistance Vs. Deficiency. Here, the problem is not routine type 1 or type 2 diabetes physiology. It is unregulated hormone release from a tumor. Many lesions are small and many are benign, but even a small lesion can cause major symptoms because the hormone effect is strong.
Because repeated lows often improve after eating, some people start snacking more often or gain weight before the cause is identified. Others notice symptoms mainly after long gaps between meals. The main danger is not usually the size of the mass. It is the ongoing risk of recurrent low glucose.
Why it matters: Repeated low glucose can impair driving, work, judgment, and memory before the cause is identified.
Common Symptoms and When They Can Be Dangerous
Most symptoms come from hypoglycemia rather than the tumor mass itself. The body first reacts with stress-hormone symptoms, and then the brain begins to run short on glucose.
Early Autonomic Signs
Early symptoms may include sweating, tremor, hunger, anxiety, palpitations, weakness, headache, or nausea. Episodes often improve after carbohydrates. Because these events may happen between meals, the pattern can resemble the low-sugar episodes covered in Fasting Hypoglycemia or the broader comparison in Hypoglycemia Vs. Hyperglycemia.
Neuroglycopenic Signs
When the brain is deprived of glucose, neuroglycopenic symptoms (brain-related effects of low glucose) can appear. These may include blurred vision, poor concentration, irritability, confusion, slurred speech, behavior change, fainting, or seizures. Because insulinoma keeps lowering glucose between meals, morning episodes and exercise-related events are common clues. Some people are first misdiagnosed with panic attacks, migraine, alcohol intoxication, or epilepsy.
Repeated episodes may also dull a person’s warning signs over time. When that happens, confusion may show up before shakiness or hunger. That is one reason unexplained symptoms deserve an actual glucose check when possible.
Severe episodes deserve urgent attention. General safety steps in Managing Hypoglycemia and context from Diabetic Coma Vs. Insulin Shock can help explain why loss of consciousness, seizures, or inability to swallow safely should not be handled as routine symptoms.
- Seizure or collapse during a low.
- Confusion that does not quickly improve.
- Inability to swallow or protect the airway.
- Any low-sugar event while driving.
Why It Develops and Who Is at Higher Risk
In most cases, doctors cannot identify a single preventable cause. These tumors arise from insulin-producing beta cells and are often sporadic, which means they occur without a clear inherited reason. A smaller share are linked to multiple endocrine neoplasia type 1, or MEN1, an inherited syndrome associated with tumors in the pancreas, parathyroid glands, and pituitary.
Family history matters because MEN1 can involve more than one endocrine organ. A personal or family history of parathyroid disease, pituitary tumors, kidney stones related to high calcium, or other pancreatic neuroendocrine tumors may prompt a broader inherited-syndrome discussion.
Risk discussions can be confusing because many people think first about diabetes when they hear the word insulin. This is a different process. Medication-related lows and other endocrine or metabolic problems are far more common overall than a beta-cell tumor. A high-insulin blood test alone also does not prove insulinoma, because the pattern seen in Hyperinsulinemia can happen for several reasons.
Most tumors are benign. Malignant disease is less common, but it matters when imaging shows spread or when symptoms return after treatment. Prognosis usually depends on whether the tumor is localized, whether it can be removed, and whether an inherited syndrome such as MEN1 is involved.
CanadianInsulin.com operates as a prescription referral platform.
How Doctors Confirm the Diagnosis
Diagnosing insulinoma depends on documenting Whipple triad and then showing that insulin levels are inappropriately high for the glucose level. Whipple triad means symptoms consistent with hypoglycemia, a measured low plasma glucose at the time of symptoms, and relief after glucose is corrected.
If the pattern is not captured during a routine visit, clinicians may use a supervised fast. The familiar 72-hour fast test does not mean every person fasts the full three days. It is a monitored hospital-based evaluation that ends once diagnostic criteria are met or the planned observation is completed safely.
Most specialists want biochemical proof before chasing tiny lesions on scans. That matters because small pancreatic findings can be incidental and unrelated. Once the lab pattern fits, imaging becomes much more useful for treatment planning.
| Step | What Clinicians Look For | Why It Matters |
|---|---|---|
| Symptom review | Episodes during fasting, overnight, or after exertion | Builds suspicion for recurrent hypoglycemia |
| Biochemical testing | Low glucose with inappropriately high insulin, C-peptide, and proinsulin | Shows insulin is being produced inside the body |
| Medication screen | Exposure to insulin secretagogues or other glucose-lowering drugs | Helps exclude drug-related causes |
| Tumor localization | CT, MRI, endoscopic ultrasound, or other specialized studies | Guides treatment planning and surgery |
During an episode, blood tests may include glucose, insulin, C-peptide, proinsulin, beta-hydroxybutyrate, and a sulfonylurea screen. C-peptide helps distinguish insulin made by the body from injected insulin. A careful medication review matters because common medication questions, including those discussed in Metformin And Hypoglycemia and Oral Diabetes Medications, are clinically different from a tumor-driven low-glucose state.
Once labs support the diagnosis, the next job is to find the lesion. CT or MRI often comes first. If those scans do not clearly show it, endoscopic ultrasound can be especially helpful because many lesions are small. Some centers use more specialized localization studies when standard imaging is inconclusive.
Treatment Options and What to Expect
Surgery is usually the preferred treatment when the tumor is localized and removable. Depending on where it sits and whether there is one lesion or several, surgeons may remove just the tumor or a portion of the pancreas. People with MEN1 or multiple tumors often need a more individualized plan.
When surgery is not possible right away, or when disease is more advanced, care focuses on preventing further low-glucose episodes and matching therapy to the tumor pattern. Clinicians may use meal-timing strategies and medicines that reduce insulin release or blunt hypoglycemia. If disease is malignant or has spread, treatment may also involve oncology-directed systemic or liver-focused approaches.
Pathology after removal helps confirm whether the lesion is benign or malignant and how aggressive it appears. Even when symptoms improve, follow-up visits may include glucose review, repeat labs, or imaging based on the original findings. Recurrence matters most when tumors are multiple, inherited syndromes are present, or disease is not fully localized.
Where needed, prescription details may be confirmed with the prescriber.
Conditions That Can Look Similar
Several more common problems can mimic this tumor, so the differential diagnosis is essential. Clinicians may need to rule out insulin or sulfonylurea use, alcohol-related lows, adrenal insufficiency, severe liver or kidney disease, critical illness, post-bariatric hypoglycemia, and factitious hypoglycemia.
If you already live with diabetes, medication effects are usually a much likelier reason for symptoms than insulinoma. That is one reason endocrinologists review the bigger picture, including the background covered in Different Types Of Diabetes. The workup is not based on one symptom or one insulin result. It relies on timing, context, observed glucose levels, and biochemical findings during an actual event.
Getting Ready for an Endocrine or Surgical Visit
A detailed symptom record can make the workup faster and safer. Because low glucose can affect memory, notes from a family member, friend, or coworker are often useful.
Useful questions to ask include whether Whipple triad has been met, whether a supervised fast is appropriate, which imaging study is most likely to help first, and how MEN1 changes the evaluation if there is a relevant family history.
Quick tip: Bring witness descriptions if episodes involve confusion, unusual behavior, or fainting.
- Episode timing: before breakfast, overnight, or after exercise.
- Glucose data: meter readings and the time they were taken.
- Food response: whether symptoms improve after carbohydrates.
- Medication list: prescriptions, supplements, alcohol, and insulin use.
- Witness reports: speech change, confusion, collapse, or seizure activity.
- Family history: MEN1, pituitary, parathyroid, or pancreatic tumors.
- Prior records: emergency visits, labs, imaging, and discharge notes.
For broader browsing, the site’s Endocrine And Thyroid Hub and Cancer Category group related topics.
Dispensing, where permitted, is handled by licensed third-party pharmacies.
Authoritative Sources
- For a patient-friendly overview from a major health system, see Cleveland Clinic overview.
- For a professional summary of diagnosis and management, see Merck Manual Professional Edition.
- For a peer-reviewed review article, see the PMC review on diagnosis and management.
In short, this rare pancreatic tumor deserves a structured evaluation when recurrent fasting or unexplained low blood sugar causes neurologic symptoms. The key steps are documenting the low, confirming inappropriate insulin activity, locating the lesion, and matching treatment to whether disease is localized or more advanced.
This content is for informational purposes only and is not a substitute for professional medical advice.


{kind=link}
{kind=link}