
An insulinoma is a rare pancreatic neuroendocrine tumor that releases insulin even when your body does not need it. That extra insulin can drive blood sugar too low, especially after fasting, exercise, or long gaps between meals. Most are benign and many are treatable, often with surgery, but diagnosis can be slow because episodes may look like anxiety, fainting, or seizure disorders. Understanding the pattern matters because repeated hypoglycemia can affect safety, work, driving, and brain function.
Key Takeaways
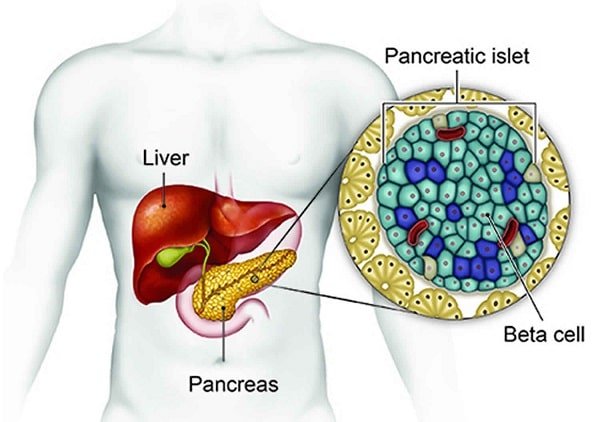
- It is a rare beta-cell tumor that causes too much insulin from inside the body.
- Symptoms usually reflect low blood sugar, not the tumor size itself.
- Diagnosis often requires documented hypoglycemia plus targeted blood tests.
- A supervised fast and imaging may be used to confirm and locate the lesion.
- Surgery is the usual definitive treatment, but urgent low blood sugar still needs prompt care.
What Insulinoma Is and Why It Causes Low Blood Sugar
Insulin comes from beta cells in the pancreas. When one of those cells becomes a tumor, it may keep secreting insulin at the wrong time. That creates endogenous hyperinsulinism (too much insulin made inside the body) and pushes glucose into tissues even while the bloodstream is already running low.
The symptoms are usually caused by hypoglycemia rather than by the lesion taking up space. In practice, that means a person may feel shaky, sweaty, hungry, or anxious first, then develop headache, blurred vision, slowed thinking, or odd behavior as the glucose level falls further. For background on glucose hormones, see Endocrine System Basics or browse the Endocrine And Thyroid Hub.
Although it sits in the pancreas, this condition is not the same as diabetes. It is a type of pancreatic neuroendocrine tumor, and most cases are small and benign. The broader lab pattern can overlap with Hyperinsulinemia, but the cause is different and the workup is more specific.
Common Symptoms and Red Flags
Symptoms usually appear when glucose falls, not when the tumor grows. Episodes often happen after an overnight fast, a missed meal, strenuous activity, or drinking alcohol without enough food. Many people feel better quickly after juice, glucose tablets, or a snack, which can make the pattern easy to overlook.
Because the brain depends heavily on glucose, some episodes look neurological rather than metabolic. Family members may notice irritability, staring spells, memory lapses, morning headaches, or behavior changes. That is one reason the condition can be mistaken for panic attacks, migraine, alcohol effects, or seizure disorders.
| Pattern | What it can look like |
|---|---|
| Early autonomic symptoms | Sweating, tremor, hunger, palpitations, anxiety, tingling, or weakness. |
| Neuroglycopenic symptoms | Confusion, blurred vision, slurred speech, irritability, poor concentration, or unusual behavior. |
| More severe episodes | Fainting, seizure, injury, or inability to safely swallow. |
Whipple Triad In Plain Language
Clinicians often look for Whipple triad: symptoms that fit hypoglycemia, a low measured plasma glucose at the same time, and improvement after glucose is corrected. The triad does not identify the cause by itself, but it helps confirm that the episode is true low blood sugar rather than a similar feeling with a normal reading.
Why it matters: Recurrent lows can affect driving, work, and independent living before a diagnosis is made.
For broader context, compare Fasting Hypoglycemia with Hypoglycemia Vs Hyperglycemia. If an episode includes loss of consciousness or seizure, urgent medical evaluation is appropriate.
Causes, Risk Factors, and Related Conditions
Most cases happen sporadically, which means there is no clear outside trigger and no obvious way the person caused it. A smaller group is linked to multiple endocrine neoplasia type 1, usually called MEN1. MEN1 is an inherited syndrome that can involve the parathyroid glands, pituitary gland, and pancreas, so a family history of endocrine tumors matters.
There is no strong evidence that everyday sugar intake, stress, or common lifestyle factors directly cause these tumors. Most people with insulinoma do not have a clear preventable risk factor. Benign and malignant lesions can produce very similar symptoms, so the intensity of sweating, confusion, or fainting does not tell you whether the tumor has spread.
This condition is only one explanation for fasting hypoglycemia. Doctors also think through insulin or sulfonylurea exposure, severe illness, alcohol-related lows, liver or kidney disease, adrenal or pituitary hormone deficiency, and other rare tumors or metabolic disorders. That wider differential diagnosis matters because treatment changes completely if the problem is medication-related or part of a broader endocrine syndrome.
That is also why it should not be confused with the glucose problems seen in Different Types Of Diabetes. Medication history remains important too, because not every low reading points to a tumor. For one common point of confusion, see Metformin And Hypoglycemia.
When required, prescription details may be confirmed with the prescriber.
How Doctors Diagnose It
Diagnosis usually starts by proving that real hypoglycemia is occurring during symptoms. Doctors begin with the history, the timing of attacks, medication review, and blood work taken during a spontaneous episode or during a monitored fast. The goal is to match symptoms to objective lab findings.
Home glucose meters can help establish timing, but diagnosis relies on lab-quality plasma testing. A personal meter reading may support the story, yet it is not enough on its own to confirm endogenous hyperinsulinism or to sort out the differential diagnosis.
Why A Supervised Fast May Be Used
The classic workup checks plasma glucose together with insulin, C-peptide, and proinsulin. A sulfonylurea screen may be added to rule out medication-related causes. When episodes do not happen often enough to catch naturally, a supervised fast lasting up to 72 hours may be done in a hospital or another controlled setting. This is not something to attempt alone at home.
Doctors suspect insulinoma when insulin remains inappropriately present while glucose falls. The supervised setting also allows safe observation for neuroglycopenia (brain-related low-glucose symptoms) and helps distinguish a tumor from injected insulin use or other causes of low sugar. In some people, symptoms appear early in the fast. In others, it takes longer to capture the pattern safely.
Imaging Comes After Biochemical Confirmation
Once the lab pattern supports the diagnosis, imaging is used to find the lesion. Depending on the case, that may include CT, MRI, endoscopic ultrasound, or specialized localization studies. Very small pancreatic lesions can be difficult to see, so a first negative scan does not always end the evaluation.
For general low-sugar response steps, see Manage Hypoglycemia. If severe episodes have occurred, the pages on Diabetic Coma and Insulin Shock Differences explain why emergency assessment matters.
Treatment and Management Options
The usual insulinoma treatment for a localized lesion is surgery. The exact procedure depends on where the tumor sits in the pancreas, how many lesions are present, and whether nearby structures are involved. When a single benign lesion can be removed completely, surgery may be definitive.
Surgical planning is individualized. Some lesions can be removed directly, while others require a wider pancreatic operation based on location and anatomy. That decision depends on localization results and specialist judgment, not on a one-size-fits-all formula.
Some people need temporary symptom control before surgery or while the workup continues. That can include planned meal timing, hospital glucose support during severe episodes, and medicines that reduce insulin release or help stabilize blood sugar. If the tumor is malignant or cannot be removed fully, treatment may expand to other specialist options, including systemic or tumor-directed therapies.
Severe hypoglycemia still needs immediate attention. Fast-acting carbohydrate may help when the person is awake and able to swallow safely. If they are confused, faint, having a seizure, or unable to take food by mouth, emergency care is needed. Some patients at risk of severe lows are prescribed rescue glucagon; the Glucagon Injection Kit page explains one form used in acute hypoglycemia.
CanadianInsulin.com is a prescription referral platform, not a dispensing pharmacy.
What Prognosis and Follow-Up Often Look Like
Most insulinoma cases are benign. When the tumor is fully removed, many people stop having repeated hypoglycemia, though follow-up still matters. Pathology results, symptom changes, and the possibility of MEN1 or more than one lesion all shape the follow-up plan.
Malignant disease is less common but more complicated. Prognosis then depends on spread, tumor biology, and response to specialist care rather than on one single rule. Follow-up may include repeat imaging, review of glucose trends, and monitoring for recurrence or ongoing nutrition issues.
Follow-up is especially important if symptoms return, labs remain abnormal, or the person has features suggesting MEN1. In those cases, clinicians may look beyond the pancreas and monitor other endocrine glands over time.
A person can feel better long before the full evaluation is finished. That improvement is reassuring, but it does not replace scheduled endocrinology or surgical review.
Practical Next Steps Before a Specialist Visit
If recurring low blood sugar is being evaluated, preparation can make the visit more useful. The aim is better documentation, not self-testing to extremes or deliberate fasting without instructions. A clear timeline often helps the care team narrow the differential diagnosis faster.
- Track the timing: Note whether episodes happen overnight, before meals, after exercise, or after alcohol.
- Record symptoms: Include sweating, tremor, confusion, vision changes, or unusual behavior.
- Save glucose readings: Bring meter or lab results if you have them.
- List all medicines: Include diabetes drugs, supplements, and any access to insulin or sulfonylureas.
- Note family history: Mention endocrine tumors, parathyroid disease, or MEN1.
- Bring prior imaging: Old CT, MRI, or ultrasound reports can prevent repeated testing.
- Ask about safety: Driving, work, and exercise plans may need short-term adjustments.
Useful questions include whether the episodes satisfy Whipple triad, whether a supervised fast is needed, which imaging study is most helpful in the next step, and what short-term safety changes make sense while the evaluation is underway.
Quick tip: Write down the last meal, the time of symptoms, and what corrected them.
Where permitted, licensed third-party pharmacies handle dispensing and fulfilment.
Authoritative Sources
- A plain-language overview is available from Cleveland Clinic.
- A professional summary can be reviewed in the Merck Manual Professional Edition.
- A detailed review article is archived at PubMed Central.
In short, insulinoma is a rare but important cause of recurrent hypoglycemia. Matching symptoms to documented low glucose, then locating the lesion with focused testing, is the core path to diagnosis and treatment. Further reading through endocrine and hypoglycemia resources can help you prepare for specialist care.
This content is for informational purposes only and is not a substitute for professional medical advice.


{kind=link}
{kind=link}