
Where is insulin produced? In the body, it is made by beta cells in the pancreas, specifically within small cell clusters called the islets of Langerhans. Those cells also store the hormone in tiny granules until rising blood glucose triggers release. Treatment insulin is different. It is produced in controlled pharmaceutical facilities, not in a human pancreas. Keeping those ideas separate helps you understand diabetes, lab terms, and why losing natural insulin production is not the same as using insulin as a medication.
Key Takeaways
- The pancreas is the organ that makes insulin.
- Beta cells in pancreatic islets produce the hormone.
- Insulin is stored in tiny cellular granules before release.
- Glucose signals help trigger insulin secretion into blood.
- Treatment insulin is manufactured through biotechnology.
Where Is Insulin Produced in the Body?
In the body, insulin comes from the pancreas, a gland that sits behind the stomach. More precisely, it is produced in the endocrine (hormone-making) part of the pancreas, not the enzyme-producing part that helps with digestion. That answer sounds simple, but the exact location matters because many blood sugar disorders begin when these hormone-making cells are damaged, stressed, or lost.
Inside the Endocrine Pancreas
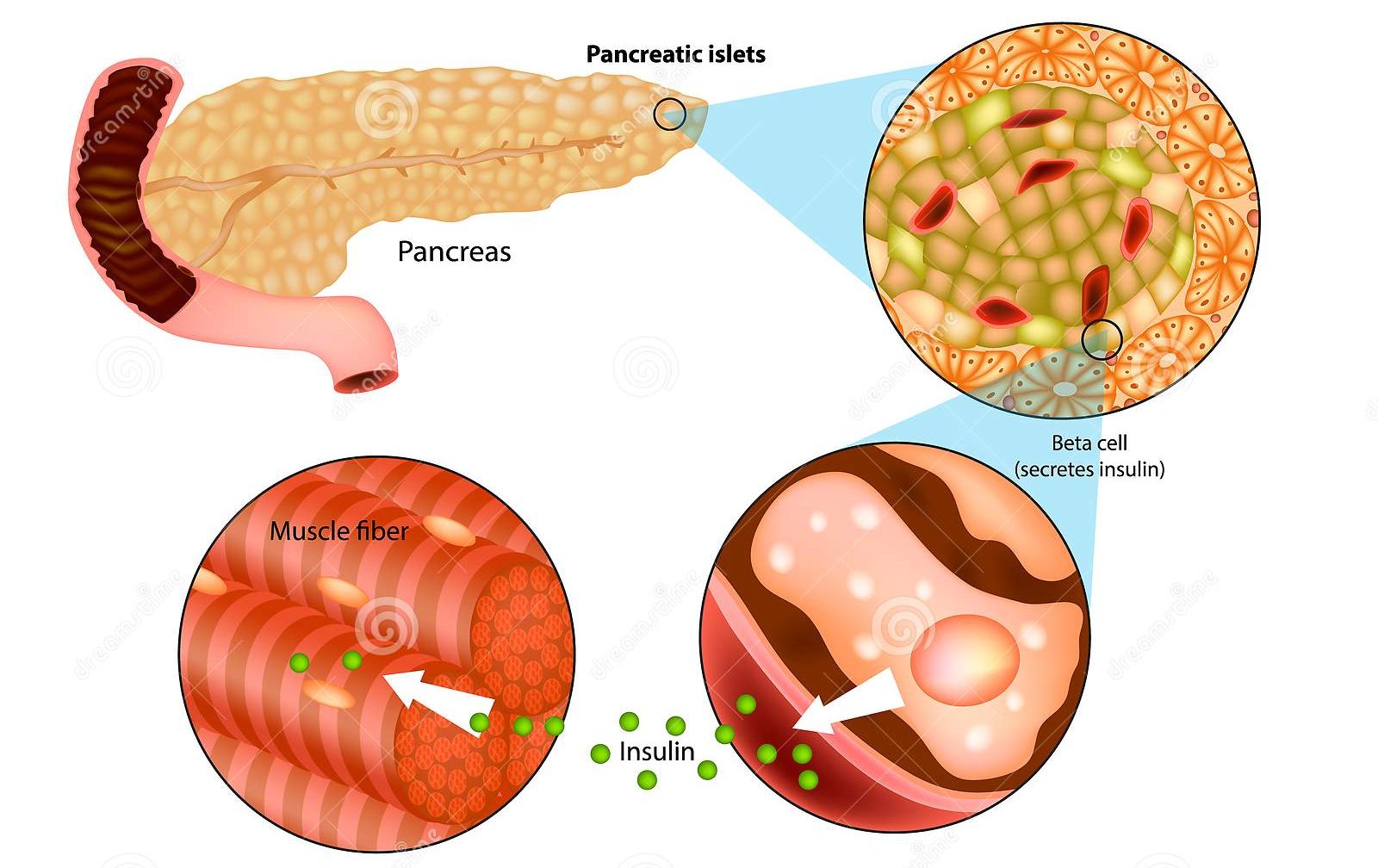
The key structures are the islets of Langerhans, small clusters of cells scattered throughout the pancreas. Beta cells in those islets make insulin. Alpha cells make glucagon, a different hormone that raises blood glucose when needed. So when someone asks which organ produces insulin, the organ is the pancreas, but the specific source is the pancreatic beta cell.
Only a small portion of the pancreas is devoted to hormone production. Most of the organ supports digestion by making enzymes. That split is important. It explains why some pancreatic problems can affect both digestion and glucose regulation at the same time, even though those functions come from different types of cells.
This is also why broad anatomy terms can be misleading. A person may still have a pancreas, yet make very little insulin if beta cells are severely damaged. For broader background on glucose control and diabetes basics, the Diabetes Articles collection gives useful context.
Why it matters: Knowing the exact source of insulin makes diabetes language much easier to follow.
How Beta Cells Make and Release Insulin
Beta cells do more than release a finished hormone. They first build insulin from precursor proteins inside the cell, then package it for later use. In other words, insulin production and insulin secretion are closely linked, but they are not the same step.
From Proinsulin to Insulin
Inside beta cells, the body assembles a precursor that is processed into proinsulin, then split into insulin and C-peptide, a linked marker of the body's own insulin output. These molecules are packed into secretory granules (tiny storage packets) inside the cell. That is why C-peptide tests can help show whether the pancreas is still making its own insulin.
Within those granules, insulin is kept in a stable stored form until the cell receives the right signal. This lets the pancreas respond quickly instead of building every molecule at the exact moment it is needed. Storage, then, is part of the normal production system rather than a separate process.
When blood glucose rises after eating, beta cells sense that change. A series of signals inside the cell leads the granules to fuse with the cell membrane and release insulin into the bloodstream. From there, insulin helps move glucose out of the blood and into tissues. If you are comparing diabetes types, T1D vs T2D is a practical place to start.
It also helps to separate where the hormone is made from where it works. The pancreas produces insulin locally. Its effects, however, are seen throughout the body, especially in the liver, muscle, and fat tissue.
Where Insulin Is Stored Before Release
Before release, insulin is stored inside beta cells, not as a large reserve floating freely in the bloodstream. The storage site is the secretory granule. These granules allow the pancreas to react quickly when glucose rises. Some hormone is ready for rapid release, while more can be made and packaged as needed.
The pancreas also releases insulin in different patterns. Small background amounts help between meals, while larger bursts follow rising glucose after eating. Stored granules make those fast bursts possible, because the cell does not have to build every molecule from scratch at the last second.
People often confuse insulin storage with glucose storage. The liver and muscles store glucose in the form of glycogen, but they do not manufacture insulin. So if you are asking where insulin is made versus where it is stored, both answers point back to beta cells inside the pancreas.
| Topic | Natural insulin in the body | Manufactured insulin for treatment |
|---|---|---|
| Where it is made | Beta cells in pancreatic islets | Controlled pharmaceutical production systems |
| Where it is stored | Secretory granules inside beta cells | Vials, cartridges, or pens after formulation |
| How it is released | Triggered by cellular glucose sensing | Given as a medication, usually by injection |
| Main purpose | Normal blood glucose regulation | Replace or supplement insulin when needed |
Quick tip: If a source mentions beta cells or islets, it is describing the body's own insulin pathway.
How Manufactured Insulin Is Made
Medical insulin is not made in a human pancreas. Today, most insulin products are produced using recombinant DNA methods, usually in bacteria or yeast. In simple terms, scientists give those cells the instructions to make human insulin or a modified insulin analog, then the protein is purified and prepared for medical use.
Natural Production vs Pharmaceutical Manufacturing
This process is very different from natural hormone production. The body makes insulin continuously in living beta cells and releases it moment by moment. Pharmaceutical manufacturing happens in tightly controlled facilities, where insulin is produced at scale, purified, tested, and formulated for use in pens, cartridges, or vials. That is what most people mean when they ask where treatment insulin gets manufactured.
At a high level, manufacturers begin with cell lines that carry the genetic instructions for insulin production. Those cells are grown in large fermentation systems, and the resulting protein goes through multiple purification steps before it becomes a finished medicine. The goal is consistency. A prescribed product has to deliver a known formulation, not the natural second-to-second variation seen inside the body.
Some older insulin products historically came from animal pancreases, but modern insulin is commonly recombinant. Some analog insulins are slightly modified so they act faster or last longer, but they are still made through biotechnology rather than by using human pancreatic tissue. In some medication pathways, dispensing is handled by licensed third-party pharmacies where local rules allow.
That difference matters because natural insulin loss and access to manufactured insulin are separate issues. One is a biological problem inside the pancreas. The other involves diagnosis, prescribing, and the medication supply process.
Why This Matters in Diabetes
In diabetes, the main problem may be reduced insulin production, poor insulin release, insulin resistance, or a combination. Type 1 diabetes usually involves severe loss of beta-cell function, so the body makes little or no insulin. T2D is different. Many people with T2D still produce insulin, especially early on, but their tissues do not respond to it well enough.
That is why Insulin Resistance vs Insulin Deficiency is such an important distinction. Deficiency means the pancreas is not producing enough hormone. Resistance means the hormone is present, but the body is not using it efficiently. In real life, both problems can exist together.
Low insulin output does not happen only in classic T1D. It can also occur after pancreatic inflammation, certain surgeries, or other disorders that damage hormone-producing tissue. On the other hand, a person can have normal or even high insulin levels and still run high glucose if resistance is the bigger problem. That is one reason lab results and symptoms need clinical context.
Over time, beta cells may struggle to keep up with rising demand. That is one reason Obesity And T2D and the T2D Hub often discuss both resistance and pancreatic workload. Some people with T2D eventually need insulin therapy, which is covered in When T2D Needs Insulin.
Problems with insulin production or insulin action can push glucose too high or, less commonly, contribute to lows in specific situations. For symptom context, see High Blood Sugar Signs or review Hypoglycemia vs Hyperglycemia. Those topics do not focus on pancreatic anatomy, but they show what can happen when insulin balance is off.
Common Mix-Ups About Insulin Production
Several terms sound similar, so confusion is common. A few distinctions clear up most of the problem.
- The liver makes insulin: No. The liver stores and releases glucose, but beta cells make insulin.
- All pancreatic cells make insulin: No. Only specific endocrine cells do that job.
- Injected insulin comes from the pancreas: No. Treatment insulin is manufactured separately.
- Diabetes always means zero insulin: No. Many people, especially with T2D, still make some insulin.
- Insulin is stored like body fat: No. It is stored in tiny cellular granules before release.
Another easy mix-up is the difference between insulin and glucagon. Both come from the pancreas, but they do opposite jobs. Insulin lowers blood glucose by helping tissues take in and use glucose. Glucagon raises blood glucose when levels fall too low. Understanding both hormones makes the pancreas easier to understand as a control center rather than a single-purpose organ.
Related Reading and Next Steps
If you came here asking about insulin production, the short answer is still the same: pancreatic beta cells make the body's insulin. The next useful question, though, is often whether the body is making enough, releasing it normally, or responding to it properly. That is where treatment discussions become more individualized.
For broader education, browse T2D Articles, the Diabetes Medications hub, or the general Diabetes Hub. Those pages can help connect anatomy, symptoms, and treatment options without reducing the topic to a single organ.
Some people explore cash-pay or cross-border fulfilment when eligibility and local rules allow.
In short, the pancreas makes insulin, beta cells store it until release, and medical insulin is produced separately through biotechnology. Keeping those three ideas distinct makes diabetes language much easier to follow.
Authoritative Sources
- For a patient-friendly overview of insulin, Cleveland Clinic on insulin
- For hormone roles within the pancreas, Endocrine Society on pancreas hormones
- For background on commercial insulin development, American Chemical Society on insulin development
This content is for informational purposes only and is not a substitute for professional medical advice.


{kind=link}
{kind=link}